“Penyelam yang menderita penyakit dekompresi memiliki prevalensi patent foramen ovale (PFO) dua kali lipat dari populasi pada umumnya.”
Memiliki katup jantung yang sehat sangat penting jika jantung Anda ingin memompa dan mengedarkan darah dengan benar ke seluruh tubuh Anda. Beberapa orang dilahirkan dengan kelainan struktural di katup jantung atau di dindingnya. Banyak gangguan seperti itu didiagnosis di awal kehidupan dan diperbaiki, memulihkan kapasitas latihan individu yang terkena dan memungkinkan mereka untuk menyelam dengan aman. Namun, beberapa kelainan struktural bawaan, seperti kondisi yang dikenal sebagai foramen ovale paten, mungkin tidak menjadi jelas sampai setelah individu yang terkena mulai menyelam — dan dapat mengakibatkan peningkatan risiko cedera menyelam tertentu. Selain itu, beberapa orang di kemudian hari terkena dampak kerusakan katup yang didapat yang dapat memengaruhi kebugaran mereka untuk menyelam.
Dalam bab ini, Anda akan belajar tentang:
Gambaran Umum Gangguan Katup (Valvular Disorder)
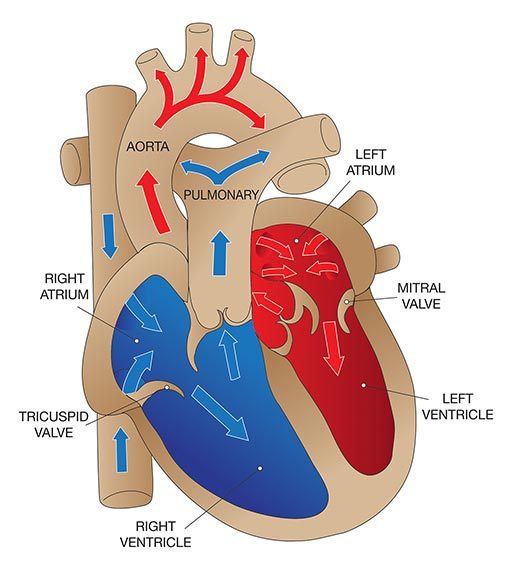
Jantung memiliki empat katup utama yang memfasilitasi aktivitas pemompaan jantung:
- Katup trikuspid, antara atrium kanan dan ventrikel kanan.
- Katup pulmonal, antara ventrikel kanan dan arteri pulmonalis.
- Katup mitral, antara atrium kiri dan ventrikel kiri.
- Katup aorta, antara ventrikel kiri dan aorta.
Setiap katup terdiri dari satu set penutup (juga disebut "selebaran" atau "puncak") yang membuka dan menutup untuk memungkinkan darah mengalir ke arah yang benar. Fungsi katup dapat terganggu oleh kelainan bawaan atau didapat. Kerusakan pada katup dapat terjadi karena infeksi, demam rematik atau penuaan. Misalnya, lubang di katup mungkin menyempit (kondisi yang dikenal sebagai "stenosis"), yang berarti jantung harus bekerja lebih keras untuk mendapatkan darah melalui lubang tersebut; ini menghasilkan tekanan yang lebih tinggi di dalam jantung dan akhirnya menyebabkan otot jantung berkembang secara berlebihan. Masalah katup umum lainnya adalah penutupan tidak lengkap, yang memungkinkan darah mengalir mundur melalui katup (kondisi yang dikenal sebagai "regurgitasi"); ini membebani jantung dengan darah, yang akhirnya mengakibatkan pembesaran (atau "dilatasi") rongga jantung.
Dua gangguan katup yang paling umum pada orang dewasa yang lebih tua adalah stenosis aorta dan regurgitasi mitral. Gejala gangguan katup bervariasi tergantung pada katup mana yang terpengaruh serta pada jenis dan tingkat keparahan perubahan. Perubahan ringan mungkin tidak menimbulkan gejala; murmur jantung - terdeteksi saat jantung diperiksa dengan stetoskop - sering kali merupakan tanda pertama kerusakan katup. Namun, pada stenosis aorta, pengerahan tenaga dapat menyebabkan nyeri dada (dikenal sebagai "angina") atau perasaan sesak di dada, sesak napas, pingsan, atau jantung berdebar-debar. Kematian mendadak pada atlet sehat terkadang disebabkan oleh stenosis aorta. Regurgitasi juga dapat menyebabkan gejala yang dapat dideteksi, seperti sesak napas atau mengi saat berbaring; keluhan ini dapat diintensifkan dengan olahraga, peningkatan resistensi terhadap pernapasan dan perendaman.
Perawatan untuk gangguan katup umumnya melibatkan pembedahan. Katup yang rusak dapat diperbaiki atau diganti dengan katup prostetik.
Mencegah kerusakan katup, tentu saja, merupakan pendekatan terbaik. Pemeriksaan fisik rutin dapat mengungkap bukti penyakit katup awal. Dalam kasus seperti itu, pengawasan medis rutin yang ketat disarankan untuk mengidentifikasi, dan semoga memperlambat, perkembangan kerusakan.
Efek pada Menyelam
Anomali katup yang signifikan dapat menghalangi penyelaman sampai dapat dikoreksi. Bahkan setelah pembedahan korektif, harus ada penilaian terhadap faktor-faktor seperti kapasitas latihan, adanya regurgitasi residual dan kebutuhan akan antikoagulasi. Penilaian semacam itu harus mencakup pemeriksaan jantung yang terperinci dan kemampuan individu untuk berolahraga pada tingkat yang konsisten dengan menyelam, tanpa bukti iskemia, mengi, disfungsi jantung atau masalah yang dikenal sebagai "pirau kanan-ke-kiri."
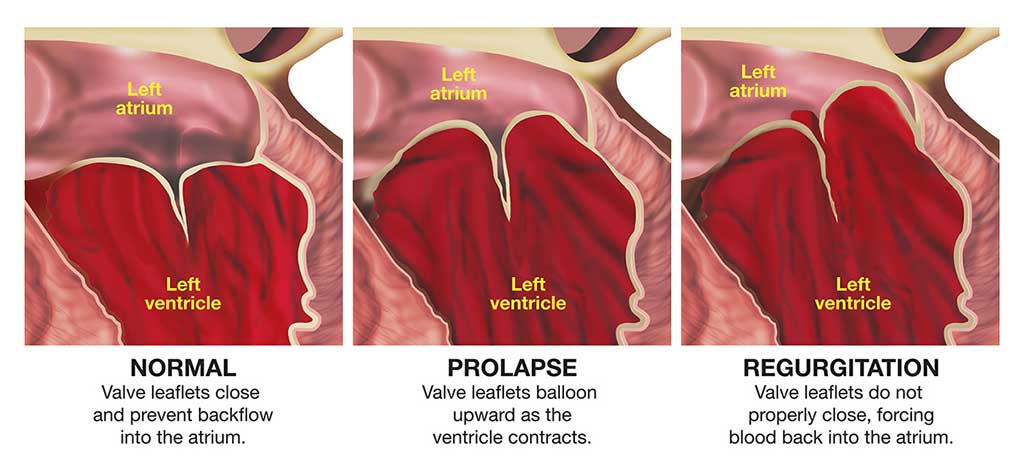
Prolaps Katup Mitral
Prolaps katup mitral (MVP) juga dapat disebut sebagai "sindrom klik-murmur" atau "sindrom floppy-valve." Ini adalah kondisi umum, terutama pada wanita. Masalah timbul sebagai akibat dari kelebihan jaringan dan jaringan ikat longgar di katup mitral jantung, sehingga bagian dari katup menonjol ke dalam ventrikel kiri setiap kali jantung berkontraksi.
Seseorang dengan MVP mungkin sama sekali tidak memiliki gejala atau mungkin menunjukkan gejala mulai dari palpitasi sesekali atau perasaan yang tidak biasa di dada saat jantung berdetak, hingga nyeri dada atau infark miokard (atau serangan jantung). MVP juga dikaitkan dengan sedikit peningkatan risiko stroke kecil (dikenal sebagai "serangan iskemik transien") atau kehilangan kesadaran sementara.
Beta blocker - obat yang biasa digunakan untuk mengobati tekanan darah tinggi - kadang-kadang diresepkan untuk prolaps katup mitral. Mereka sering menyebabkan penurunan kapasitas latihan maksimum dan juga dapat mempengaruhi saluran udara. Efek samping ini biasanya tidak menimbulkan masalah bagi rata-rata penyelam, tetapi mungkin signifikan dalam situasi darurat.
Efek pada Menyelam
Seringkali, MVP tidak menghasilkan perubahan aliran darah yang akan mencegah seseorang menyelam dengan aman. Seorang penyelam dengan MVP yang tidak memiliki gejala (yaitu, tidak ada nyeri dada, perubahan kesadaran, palpitasi atau detak jantung yang tidak normal) dan yang tidak meminum obat untuk masalah tersebut dapat berpartisipasi dengan aman dalam menyelam. Tetapi siapa pun dengan MVP yang menunjukkan irama jantung abnormal, yang dapat menyebabkan palpitasi, tidak boleh menyelam kecuali palpitasi dapat dikontrol dengan obat antiaritmia dosis rendah.
Paten Foramen Ovale
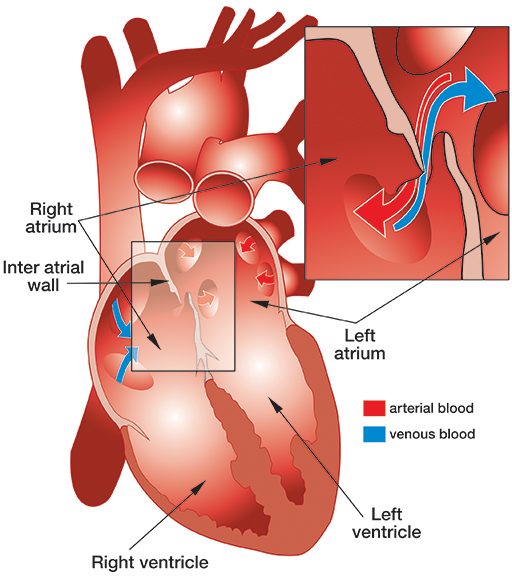
Patent foramen ovale (PFO) adalah lubang yang cukup umum, bawaan, umumnya jinak antara atrium kiri dan kanan jantung (lihat ilustrasi).
Saat janin berkembang di dalam rahim, dinding yang memisahkan atrium kiri dan kanan jantung berkembang dari septum primum, yang tumbuh ke atas, dan septum sekundum, yang tumbuh ke bawah. Septa tumpang tindih, menciptakan semacam pintu jebakan (dikenal sebagai "foramen ovale"), yang memungkinkan darah beroksigen dari plasenta ibu yang telah memasuki atrium kanan janin melewati atrium kirinya. Saat lahir, paru-paru bayi mengembang, dan tekanan yang dihasilkan di atrium kiri menutup foramen ovale. Biasanya, tak lama setelah lahir, sekering bekas pembukaan ini menutup - tetapi pada sekitar 27 persen bayi, ia gagal menyatu sepenuhnya dan menghasilkan PFO.
PFO sering tidak menimbulkan gejala, dan kebanyakan orang yang memilikinya tidak pernah menyadari faktanya. PFO didiagnosis dengan menyuntikkan sejumlah kecil udara ke dalam vena dan mengamati perjalanannya melalui jantung menggunakan ekokardiografi. Ada dua metode ekokardiografi. Ekokardiografi transtorasik (TTE) mudah dan non-invasif — hanya melibatkan penempatan probe ultrasound di dinding luar dada — tetapi mendeteksi PFO hanya pada 10 persen hingga 18 persen populasi — sekitar setengah dari mereka yang mungkin memilikinya. Ekokardiografi transesofageal (TEE) - yang melibatkan anestesi lokal dan sedasi intravena, sehingga probe dapat dimasukkan ke dalam kerongkongan - mendeteksi PFO pada 18 persen hingga 33 persen populasi. Namun, meskipun TEE lebih sensitif daripada TTE, masih banyak hasil negatif palsu dengan kedua teknik tersebut; TTE yang dilakukan dengan benar mungkin sebenarnya lebih andal daripada TEE.
Salah satu perawatan paling umum untuk PFO adalah prosedur yang disebut penutupan transkateter; ini melibatkan pemasangan kateter melalui selangkangan dan naik ke vena femoralis ke dalam jantung, di mana alat yang disebut occluder ditanamkan di seluruh PFO. Occluder datang dalam berbagai bentuk dan bentuk, tetapi sebagian besar bertindak seperti payung ganda yang terbuka di setiap sisi dinding atrium dan menutup lubang. Seiring waktu, jaringan tumbuh di atas ocluder dan menutupi permukaannya sepenuhnya. Implantasi dilakukan dengan anestesi lokal dan sedasi intravena, dan pasien tetap sadar. Dibutuhkan kurang dari satu jam dan dapat dilakukan dengan rawat jalan atau menginap satu malam. Kebanyakan pasien dapat kembali ke aktivitas normal mereka dalam dua hari, tetapi mereka harus minum obat antikoagulan dan/atau antiplatelet selama tiga sampai enam bulan. Pembatasan pasca operasi lainnya termasuk tidak ada perawatan gigi elektif (seperti pembersihan) selama tiga bulan, tidak ada olahraga kontak selama tiga bulan dan tidak ada angkat berat selama satu minggu. Seorang penyelam yang menjalani penutupan transkateter PFO harus tidak melakukan penyelaman selama tiga sampai enam bulan.
Tidak ada data yang tersedia tentang hasil penutupan PFO pada penyelam. Tetapi hasil berikut dicatat pada pasien yang menjalani penutupan PFO untuk pencegahan stroke (namun, perhatikan bahwa pasien ini memiliki kondisi medis yang mendasari yang dapat berkontribusi pada risiko hasil buruk yang lebih besar dari rata-rata):
- Keberhasilan: Penutupan saluran lengkap dicapai pada 95 persen kasus dan penutupan tidak lengkap pada 4 hingga 5 persen kasus; tidak ada perbaikan yang ditunjukkan hanya pada 1 persen kasus.
- Komplikasi: Kematian keseluruhan kurang dari 1/10 dari 1 persen (0,093 persen). Kebutuhan untuk operasi tindak lanjut karena kejadian buruk yang terkait dengan perangkat kurang dari 1 persen (0,83 persen).
- Komplikasi serius: Angka kejadian kematian, stroke, infeksi, perdarahan atau cedera pembuluh darah sebesar 0,2 persen; pergerakan atau pelepasan alat, 0,25 persen; pembentukan bekuan pada perangkat, 0,3 persen; komplikasi utama pada periode perioperatif, 1,2 persen; dan komplikasi jangka menengah ringan, 2,4 persen.
Efek pada Menyelam
Penyelam yang menderita penyakit dekompresi (DCS) memiliki prevalensi PFO dua kali lipat dari populasi pada umumnya. Dan pada penyelam yang menunjukkan gejala DCS neurologis, prevalensi PFO empat kali lebih besar. Risiko DCS tampaknya meningkat dengan ukuran PFO. Berdasarkan fakta-fakta ini, diasumsikan bahwa penyelam dengan PFO memiliki risiko DCS yang lebih besar daripada mereka yang tidak memiliki PFO; namun, satu-satunya studi prospektif yang dirancang untuk secara langsung mengukur risiko relatif DCS pada penyelam dengan PFO masih berlangsung.
Berikutnya Bab 4 – Penyakit Jantung Iskemik >