Telinga adalah organ kompleks yang memungkinkan orientasi dalam ruang, aktivitas fisik sehari-hari, dan komunikasi sosial. Sementara anatomi telinga mungkin menakutkan sampai batas tertentu, kami telah mencoba memberikan gambaran yang disederhanakan namun jelas untuk meningkatkan pemahaman Anda tentang proses penting untuk menyelam.
Penyamaan tekanan di telinga tengah adalah keterampilan yang paling penting bagi penyelam. Jika tidak dikuasai dengan baik, penyelam bisa terluka dan terkadang cacat permanen. Pada penyelam dengan telinga yang sehat, barotrauma telinga dapat dicegah. Penyelam harus menginvestasikan waktu dan upaya untuk menguasai teknik penyamaan tekanan (ekualisasi).
Telinga adalah organ pendengaran dan keseimbangan. Ini terdiri dari rongga dalam struktur tengkorak yang dilapisi dengan jaringan lunak, yang membungkus tiga ruang khusus yang diisi dengan udara atau cairan (telinga luar, tengah dan dalam); ruang-ruang khusus ini menampung mekanisme transmisi suara dan aparatus sensorik.
Struktur
Telinga luar meliputi pinna (daun telinga) dan saluran telinga hingga gendang telinga (membran timpani), yang memisahkannya dari telinga tengah. Lapisan telinga luar adalah kulit yang kaya dengan kelenjar yang menghasilkan kotoran telinga.
Telinga tengah adalah rongga di tulang temporal yang dilapisi dengan lapisan tipis jaringan yang mirip dengan yang ditemukan di hidung dan tenggorokan. Ini dipisahkan dari saluran telinga oleh gendang telinga dan terhubung ke tenggorokan melalui tabung Eustachius. Ini mencakup tiga tulang kecil (tulang pendengaran) yang membentuk rantai yang melekat pada gendang telinga di satu sisi dan ke membran jendela oval di sisi telinga bagian dalam. Ruang telinga tengah diisi dengan udara pada tekanan sekitar, yang perlu disetarakan ketika tekanan sekitar berubah (seperti yang terjadi pada menyelam atau terbang). Hal ini dicapai dengan menggerakkan udara masuk atau keluar melalui tabung Eustachius, yang menghubungkan tenggorokan ke telinga tengah, menggunakan teknik pemerataan seperti manuver Valsava.
Telinga bagian dalam, atau labirin, termasuk koklea (organ pendengaran) dan vestibulum dan saluran setengah lingkaran (organ keseimbangan). Koklea dan ruang depan adalah asal saraf pendengaran dan vestibular.
Fungsi
Gelombang tekanan yang ditransmisikan oleh udara atau air disalurkan oleh pinna dan liang telinga ke membran timpani. Gelombang tekanan menyebabkan membran timpani bergetar, yang menyebabkan tulang-tulang pendengaran bergerak secara simultan sebagai respons. Stapes (tulang terakhir dalam rantai) mengenai jendela oval koklea. Karena ini adalah sistem tertutup, ketika jendela oval didorong ke dalam, jendela bundar mendorong ke luar. Cairan di dalam koklea mengirimkan gelombang tekanan ke saraf pendengaran, yang pada gilirannya, mengirimkan sinyal ke otak yang ditafsirkan sebagai suara.
Bagian dari ruang depan adalah proyeksi yang dikenal sebagai kanal setengah lingkaran. Cairan dalam sistem ini bergerak sesuai dengan gerakan kepala. Di dalam kanalis semisirkularis terdapat struktur seperti rambut yang disebut silia. Silia mendeteksi pergerakan cairan melalui kanal dan mengirim sinyal melalui saraf vestibular ke otak, di mana gerakan tersebut ditafsirkan dan digunakan untuk membantu menentukan posisi kepala dalam ruang tiga dimensi.
Ekualisasi Telinga Bagian Tengah
Pemerataan telinga tengah adalah keterampilan dasar penyelam yang diperlukan yang memungkinkan pemerataan tekanan di sinus dan ruang telinga tengah dengan tekanan sekitar.
Prosedur dalam Praktek
Saat penyelam turun di kolom air, tekanan lingkungan meningkat secara linier dengan kecepatan satu setengah pon per inci persegi (PSI) untuk setiap kaki (0,1 kg/cm2)2 untuk setiap meter) dan mentransmisikan ke seluruh jaringan dan cairan tubuh. Hukum Boyle menjelaskan bagaimana volume gas berkurang ketika tekanan meningkat, jika jumlah (massa) gas dan suhu tetap sama. Telinga tengah adalah rongga kaku kecuali gendang telinga. Jadi ketika tekanan meningkat, satu-satunya cara untuk menurunkan volume adalah membungkuk gendang telinga ke arah rongga telinga tengah (kecuali jika gas ditambahkan ke ruang). Setelah gendang telinga meregang hingga batasnya, pengurangan lebih lanjut volume rongga telinga tengah tidak mungkin dilakukan; jika penurunan berlanjut, tekanan di rongga telinga tengah tetap lebih rendah dari sekitarnya. Perbedaan tekanan yang kecil akan menyebabkan kebocoran cairan dan perdarahan dari gendang telinga dan mukosa yang melapisi rongga telinga tengah (barotrauma telinga O’Neil grade 1). Ketika perbedaan tekanan mencapai 5 PSI (0,35 bar), gendang telinga dapat pecah pada beberapa penyelam; pada perbedaan tekanan lebih besar dari 10 PSI (0,75 bar), pecah akan terjadi pada sebagian besar penyelam (barotrauma telinga O'Neil grade 2). Selain itu, perubahan tekanan yang tiba-tiba dan besar dapat menyebabkan cedera telinga bagian dalam.
Jadi sekarang Anda mengerti mengapa saat turun Anda harus membiarkan lebih banyak gas masuk ke telinga tengah Anda untuk menjaga volume gas tetap konstan dan menyamakan tekanan. Telinga tengah yang normal hanya memiliki satu komunikasi fisik dengan sumber gas tambahan, yaitu tuba Eustachius yang menghubungkan rongga hidung (rhinopharynx). Dalam keadaan normal, saluran Eustachius tertutup, tetapi setiap kali kita menelan atau menguap, otot-otot di tenggorokan kita memungkinkan pembukaan sementara kecil yang cukup untuk ventilasi telinga tengah kita dan mengkompensasi tekanan.
Tidak ada yang lebih menantang telinga dan tuba Eustachius kita selain menyelam scuba dan menyelam tahan napas. Untuk menjadi penyelam scuba yang aman dan menghindari cedera telinga tengah, penting bagi Anda untuk memahami efek hukum Boyle dan belajar bagaimana secara aktif membiarkan udara masuk ke telinga tengah Anda melalui saluran Eustachius. Di bagian berikut, Anda akan menemukan teknik pemerataan yang berbeda untuk Anda coba.
Saat pendakian, tekanan di sekitarnya berkurang dan tekanan di tengah tetap lebih tinggi jika gas tidak bisa keluar dari rongga telinga tengah. Ketika tekanan di telinga tengah melebihi tekanan di sekitarnya sebesar 15-80 sentimeter air (cm H2O) yang sesuai dengan pendakian di air 0,5-2,5 kaki, tabung Eustachius terbuka, dan kelebihan gas keluar. Jika telinga Anda tidak menyamakan pada tingkat yang sama dan perbedaan tekanan mencapai sekitar 66 cm H2O (2 kaki), vertigo karena stimulus tekanan yang tidak seimbang (vertigo alternobarik) dapat terjadi.
Infeksi saluran pernapasan atas, hay fever, alergi, obat-obatan yang mendengus, merokok atau septum hidung yang menyimpang dapat mengganggu pemerataan tekanan. Jika digunakan dengan benar, teknik berikut ini efektif pada telinga tengah dan tekanan sinus pada subjek yang sehat.
Teknik Pemerataan Tekanan (Ekualisasi)
Pasif: Tidak membutuhkan usaha. Terjadi selama naik ke permukaan.
Pembukaan tuba secara sukarela: Cobalah menguap atau menggoyangkan rahang Anda. 30 persen penyelam berhasil menguasai teknik ini.
Manuver Valsava: Jepit lubang hidung Anda, dan tiup dengan lembut melalui hidung Anda.
Manuver Toynbee: Jepit lubang hidung dan menelan (teknik yang baik jika ekualisasi diperlukan selama naik).
Manuver Frenzel: Jepit lubang hidung sambil mengencangkan otot tenggorokan, dan buat bunyi huruf “k”.
Teknik Lowry: Jepit lubang hidung Anda, dan dengan lembut coba hembuskan udara dari hidung Anda saat menelan (pikirkan manuver Valsava sesuai dengan manuver Toynbee).
Teknik Edmonds: Dorong rahang Anda ke depan, dan lakukan manuver Valsava atau manuver Frenzel.
Manuver Toynbee adalah teknik yang efektif untuk menyamakan telinga Anda selama naik ke permukaan
Kiat untuk Ekualisasi
Sebelum turun, saat Anda mengapung secara netral tanpa udara di perangkat kontrol daya apung (BCD), kembangkan telinga Anda dengan lembut dengan salah satu teknik yang tercantum. Ini memberi Anda sedikit udara ekstra di telinga tengah dan sinus saat Anda turun.
Turun dengan kaki terlebih dahulu, jika memungkinkan. Hal ini memungkinkan udara untuk melakukan perjalanan ke atas ke dalam tabung Eustachius dan telinga tengah, arah yang lebih alami. Gunakan tali pemandu atau tali jangkar untuk mengontrol kecepatan turun.
Kembangkan telinga Anda dengan lembut setiap beberapa kaki selama 10 hingga 15 kaki pertama.
Sakit tidak dapat diterima. Jika ada rasa sakit, Anda telah turun tanpa menyamakan tekanan secara memadai. Naik beberapa kaki sampai rasa sakitnya berhenti.
Jika Anda tidak merasakan telinga Anda terbuka, berhentilah dan coba lagi; Anda mungkin perlu naik beberapa kaki untuk mengurangi tekanan di sekitar Anda. Jangan memantul ke atas dan ke bawah.
Mungkin berguna untuk memiringkan telinga yang tersumbat ke arah permukaan.
Jika Anda tidak dapat menyamakan tekanan, batalkan penyelaman. Konsekuensi dari turun tanpa menyamakan tekanan dapat merusak keseluruhan perjalanan menyelam atau menyebabkan kerusakan permanen dan gangguan pendengaran.
Dekongestan dan semprotan hidung dapat digunakan sebelum menyelam untuk mengurangi pembengkakan di saluran hidung dan telinga. Jika dokter Anda setuju dengan keputusan Anda untuk menggunakan dekongestan, minumlah satu hingga dua jam sebelum turun. Mereka harus bertahan dari delapan hingga 12 jam, jadi Anda tidak perlu mengambil dosis kedua sebelum penyelaman berulang. Semprotan hidung harus digunakan sekitar 30 menit sebelum turun dan biasanya berlangsung 12 jam. Berhati-hatilah saat menggunakan semprotan hidung yang dijual bebas; penggunaan berulang dapat menyebabkan reaksi rebound yang mengakibatkan peningkatan sumbatan dan kemungkinan hambatan terbalik saat pendakian ke permukaan. Dekongestan mungkin memiliki efek samping. Jangan menggunakannya sebelum menyelam jika Anda tidak memiliki pengalaman sebelumnya.
Jika sewaktu-waktu selama menyelam Anda merasa sakit, mengalami vertigo atau kehilangan pendengaran mendadak, batalkan penyelaman. Jika gejala ini berlanjut, jangan menyelam lagi dan konsultasikan dengan dokter Anda.
Cedera telinga adalah penyebab utama morbiditas di antara penyelam scuba. Cedera yang paling umum adalah barotrauma telinga tengah (MEBT). Sebagian besar kasus MEBT ringan, sembuh secara spontan, dan tidak pernah dilaporkan. Dalam kasus yang lebih serius, penyelam mencari pertolongan medis, dan beberapa menghubungi DAN. Berbagai survei menunjukkan bahwa lebih dari 50 persen dari semua penyelam mengalami MEBT setidaknya sekali. Sebaliknya, hanya 4,4 persen penyelam yang mengalami DCS seumur hidupnya.
Penyelam dapat mengalami berbagai cedera telinga lainnya, yang sebagian besar dapat dicegah, yang dirinci dalam bab berikutnya.
Barotrauma telinga tengah adalah akumulasi cairan dan darah di telinga tengah atau pecahnya gendang telinga akibat kegagalan penyetaraan tekanan di ruang udara telinga tengah selama menyelam atau terbang.
Mekanisme
Tekanan udara dalam rongga timpani - ruang berisi udara di telinga tengah - harus disamakan dengan tekanan lingkungan sekitar. Tuba Eustachius menghubungkan tenggorokan dengan rongga timpani dan menyediakan jalan untuk gas ketika diperlukan penyetaraan tekanan. Pemerataan ini biasanya terjadi dengan sedikit atau tanpa usaha. Berbagai manuver, seperti menelan atau menguap, dapat memfasilitasi proses ini.
Sumbatan pada tuba Eustachius dapat menyebabkan ketidakmampuan untuk mencapai keseimbangan, terutama saat turun, ketika tekanan berubah dengan cepat. Jika tekanan dalam rongga timpani lebih rendah daripada tekanan jaringan di sekitarnya, ketidakseimbangan ini menyebabkan ruang telinga tengah menjadi hampa udara. Hal ini menyebabkan jaringan membengkak, gendang telinga menonjol ke dalam, kebocoran cairan dan pendarahan pada pembuluh darah yang pecah. Pada titik tertentu, upaya aktif untuk menyeimbangkannya akan sia-sia, dan manuver Valsava yang kuat dapat melukai telinga bagian dalam. Pada akhirnya, gendang telinga dapat pecah; hal ini mungkin dapat meredakan rasa sakit yang berhubungan dengan MEBT, tetapi ini adalah hasil yang harus dihindari jika memungkinkan.
Faktor-faktor yang dapat berkontribusi terhadap perkembangan MEBT antara lain adalah flu biasa, alergi, atau peradangan - kondisi yang dapat menyebabkan pembengkakan dan dapat menyumbat tuba Eustachius. Teknik pemerataan yang buruk atau penurunan yang terlalu cepat juga dapat berkontribusi terhadap perkembangan MEBT.
Manifestasi
Penyelam yang tidak dapat menyamakan tekanan telinga tengah saat turun akan merasakan ketidaknyamanan pada telinga mereka (telinga tersumbat, telinga tersumbat) yang dapat berkembang menjadi nyeri hebat. Penurunan lebih lanjut hanya akan memperparah rasa sakit telinga, yang segera diikuti oleh penumpukan cairan serosa dan pendarahan di telinga tengah. Dengan penurunan lebih lanjut, gendang telinga dapat pecah, sehingga menimbulkan rasa sakit; pecahnya gendang telinga ini dapat menyebabkan vertigo, gangguan pendengaran, dan infeksi.
Penanganan
Saat menyelam: Ketika merasakan ketidaknyamanan telinga saat turun, Anda harus berhenti turun dan mencoba menyamakannya. Jika perlu, naiklah beberapa meter untuk melakukan penyetaraan. Jika penyetaraan tidak dapat dicapai, Anda harus mengakhiri penyelaman dengan aman.
Pertolongan pertama: Jika merasa telinga terasa penuh setelah menyelam, hindari menyelam lebih lanjut. Gunakan semprotan atau obat tetes dekongestan hidung. Hal ini akan mengurangi pembengkakan mukosa hidung dan mukosa tuba Eustachius, yang dapat membantu membuka tuba Eustachius dan mengeluarkan cairan dari telinga tengah. Jangan memasukkan obat tetes ke dalam telinga Anda.
Pengobatan: Segera periksakan diri ke dokter jika keluar cairan atau darah dari liang telinga, atau jika nyeri dan rasa penuh pada telinga berlangsung lebih dari beberapa jam. Jika terjadi vertigo dan pusing, yang mungkin merupakan gejala barotrauma telinga bagian dalam, Anda harus segera memeriksakan diri. Vertigo dan mual yang parah setelah menyelam memerlukan perawatan medis darurat.
Kebugaran Untuk Menyelam
Kembali menyelam dapat dipertimbangkan jika dokter menyatakan bahwa cedera telah sembuh dan tuba Eustachius berfungsi dengan baik.
Pencegahan
Jangan menyelam saat hidung tersumbat atau kedinginan.
Turunlah perlahan-lahan. Jika tidak dapat menyamakan kedudukan setelah beberapa kali mencoba, akhiri penyelaman dengan aman untuk menghindari cedera yang signifikan yang dapat menghalangi Anda untuk menyelam di sisa minggu itu.
Perforasi membran timpani adalah robekan pada gendang telinga, yang dapat terjadi saat menyelam scuba karena kegagalan penyamaan tekanan telinga tengah.
Mekanisme
Membran timpani (TM) adalah jaringan yang memisahkan telinga luar dengan ruang telinga tengah. Membran ini melekat pada rantai tulang kecil (ossicles pendengaran) yang terletak di telinga tengah. TM juga berfungsi sebagai pembatas antara ruang telinga tengah yang steril dan lingkungan sekitar.
Gendang telinga pecah dapat disebabkan oleh turunnya gendang telinga tanpa menyamakan tekanan di telinga tengah, oleh manuver Valsava yang kuat, ledakan, pukulan pada telinga/kepala, atau trauma akustik. Biasanya disertai dengan rasa sakit; ruptur mengurangi tekanan (dan rasa sakit) di telinga tengah dan dapat diikuti oleh vertigo. Mungkin terdapat perdarahan di saluran telinga.
Faktor-faktor yang berkontribusi termasuk kemacetan, pelatihan yang tidak memadai, dan tingkat penurunan yang berlebihan.
Manifestasi
Nyeri telinga saat turun yang berhenti tiba-tiba
Keluar cairan bening atau darah dari telinga
Gangguan pendengaran
Telinga berdenging (tinnitus)
Sensasi berputar (vertigo)
Mual atau muntah yang dapat diakibatkan oleh vertigo
Penanganan
Sebagian besar gendang telinga yang berlubang akan sembuh secara spontan dalam beberapa minggu. Mungkin perlu dilakukan penanganan hidung tersumbat dan sinus. Jika robekan atau lubang pada gendang telinga Anda tidak sembuh dengan sendirinya, perawatan akan melibatkan prosedur untuk menutup perforasi. Prosedur ini dapat meliputi:
Tambalan gendang telinga: Dokter spesialis THT dapat menutup robekan atau lubang dengan tambalan kertas. Ini adalah prosedur kantor di mana THT mengoleskan bahan kimia ke tepi robekan untuk merangsang pertumbuhan dan kemudian menempelkan tambalan kertas di atas lubang untuk memberikan struktur pendukung bagi pertumbuhan jaringan gendang telinga.
Pembedahan: Cacat gendang telinga yang besar dapat diperbaiki dengan pembedahan (timpanoplasti). Dokter bedah THT akan mengambil sepetak kecil jaringan Anda dan menanamnya di atas lubang di gendang telinga. Prosedur ini dilakukan secara rawat jalan, yang berarti Anda biasanya dapat pulang pada hari yang sama, kecuali jika kondisi medis Anda memerlukan rawat inap yang lebih lama di rumah sakit.
Untuk rujukan THT di daerah Anda, email Medic@DAN.org atau hubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Kebugaran Untuk Menyelam
Jika dokter Anda merasa penyembuhan sudah mantap dan tidak ada bukti adanya masalah tuba Eustachius, Anda dapat kembali menyelam dalam waktu beberapa bulan. Perforasi kronis yang tidak kunjung sembuh merupakan kontraindikasi untuk menyelam.
Pencegahan
Jangan menyelam saat terjadi kemacetan. Pertahankan kecepatan turun yang nyaman, dan samakan sesuai kebutuhan.
Sistem Penilaian O'Neill
Sistem penilaian O'Neill adalah cara baru untuk menilai tingkat keparahan barotrauma telinga tengah. Sistem ini disederhanakan dan diharapkan dapat memberikan diagnosis yang lebih konsisten dengan rincian yang cukup untuk mengarahkan pengobatan.
Kelas 0 Disfungsi Tuba Eustachius
Foto dasar yang menggambarkan penampilan anatomi TM sebelum terpapar tekanan
Gejala tanpa perubahan anatomis (tidak ada trauma) sejak awal
Kelas 1 Barotrauma
Eritema meningkat dari awal
Perangkap cairan atau udara (gelembung yang terlihat) di ruang telinga tengah
Kelas 2 Barotrauma
Perdarahan apa pun yang terjadi di dalam membran timpani atau ruang telinga tengah
Perforasi
Barotrauma Telinga Bagian Dalam
Barotrauma telinga dalam adalah kerusakan pada telinga bagian dalam akibat perbedaan tekanan yang disebabkan oleh pemerataan yang tidak sempurna atau paksa. Kebocoran cairan telinga bagian dalam dapat terjadi atau tidak.
Mekanisme cedera
Telinga bagian dalam dipisahkan dari dunia luar oleh telinga tengah. Ini adalah organ untuk pendengaran dan keseimbangan. Ketika tekanan di ruang telinga tengah disamakan dengan benar, risiko barotrauma telinga dalam sangat rendah.
Jika tekanan di telinga tengah tidak disamakan saat turun, tekanan air pada gendang telinga akan berpindah ke dalam melalui gendang telinga tengah ke jendela oval, dan jendela bundar akan menonjol ke luar. Tekanan itu sendiri dapat merusak struktur telinga bagian dalam yang sensitif. Jika tekanannya berlebihan, jendela oval atau, yang lebih umum, jendela bundar dapat robek, dan cairan telinga bagian dalam (perilimfa) dapat bocor ke telinga tengah (fistula perilimfa).
Manuver Valsava meningkatkan tekanan pada jaringan tengkorak dan sirkulasi, yang dapat mengirimkannya ke cairan koklea, sehingga menyebabkan gerakan keluar dari jendela bundar. Gelombang tekanan saja dapat menyebabkan kerusakan pada telinga bagian dalam tanpa pecahnya gendang telinga. Jika pecah, hilangnya cairan dari telinga bagian dalam akan menyebabkan kerusakan pada organ pendengaran dan terkadang pada organ keseimbangan. Jika kebocoran tidak segera dihentikan dengan penyembuhan spontan atau perbaikan melalui pembedahan, gangguan pendengaran permanen dapat terjadi.
Manifestasi
Para penyelam mungkin akan mengalaminya:
Vertigo berat
Gangguan pendengaran
Telinga berdenging/berdenging (tinnitus)
Gerakan mata yang tidak disengaja (nistagmus)
Kepenuhan pada telinga yang terkena
Gejala barotrauma telinga tengah hampir selalu ada. Vertigo biasanya parah dan disertai mual dan muntah. Gangguan pendengaran dapat terjadi secara menyeluruh, seketika, dan permanen, tetapi penyelam biasanya hanya kehilangan frekuensi yang lebih tinggi. Kehilangan pendengaran baru terlihat setelah beberapa jam. Anda mungkin tidak menyadari kehilangan pendengaran sampai Anda menjalani tes pendengaran.
Penanganan
Jika terjadi vertigo di bawah air, batalkan penyelaman, dan dapatkan bantuan untuk mencapai permukaan dengan aman. Berikan oksigen permukaan jika dicurigai adanya penyakit dekompresi. Penyedia pertolongan pertama harus melakukan pemeriksaan neurologis lengkap dan mencatat setiap defisit.
Barotrauma Telinga Bagian Dalam atau Penyakit Dekompresi Telinga Bagian Dalam?
Penting untuk membedakan kedua kondisi ini, karena penanganannya berbeda. Perawatan standar untuk DCS dalam bentuk apa pun adalah perawatan oksigen hiperbarik dalam ruang rekompresi; rekompresi atau perubahan tekanan apa pun dikontraindikasikan ketika kemungkinan terjadi barotrauma telinga dalam. Meskipun gejalanya serupa pada kedua kondisi tersebut, barotrauma didahului oleh kegagalan pemerataan tekanan telinga tengah dan biasanya terjadi pada awal penyelaman, sedangkan DCS terjadi karena kegagalan dekompresi pada akhir penyelaman.
Perawatan Definitif
Segera cari evaluasi oleh dokter untuk menyingkirkan DCS. Jika dokter Anda menyatakan bahwa ini bukan DCS, berkonsultasilah dengan spesialis THT yang berpengalaman menangani penyelam. Untuk mendapatkan rujukan di daerah Anda, kirimkan email ke Medic@DAN.org, atau hubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Hindari aktivitas, pemerataan telinga tengah, paparan ketinggian atau menyelam, bersin atau membuang ingus. Jangan mengonsumsi aspirin, asam nikotinat (vitamin), vasodilator atau antikoagulan lainnya. Perawatan konservatif meliputi istirahat di tempat tidur dengan posisi duduk dan menghindari aktivitas yang dapat meningkatkan tekanan intrakranial atau tekanan telinga tengah. Jika gejala tidak membaik, pembedahan mungkin diperlukan. Penyembuhan robekan (fistula) biasanya terjadi dalam waktu satu atau dua minggu. Gangguan pendengaran dapat menjadi permanen.
Kebugaran Untuk Menyelam
Evaluasi kebugaran untuk menyelam memerlukan dokter selam yang ahli dan tergantung pada tingkat kerusakan permanen serta kemungkinan cedera berulang.
Prognosis
Dalam banyak kasus, penyembuhan total terjadi secara spontan. Jika fistula muncul dan tidak segera sembuh secara spontan, pembedahan mungkin direkomendasikan. Pada beberapa kasus, telinga bagian dalam dapat mengalami kerusakan secara permanen; tubuh dapat beradaptasi dengan satu sisi yang tidak berfungsi dengan baik. Jika cedera terjadi pada telinga yang lain, situasinya bisa menjadi serius dan mungkin melibatkan masalah keseimbangan yang melumpuhkan.
Pencegahan
Pelajari teknik penyeimbangan yang lembut namun efektif, dan hindari penggunaan manuver Valsava yang agresif. Jangan menyelam ketika sedang padat.
Fistula Perilimfa
Fistula perilimfa adalah robekan pada membran timpani yang berbentuk bulat dan/atau oval, di mana cairan telinga bagian dalam (perilimfa) bocor.
Mekanisme
Kebocoran perilimfa dari labirin dapat terjadi ketika jendela bulat atau oval terganggu karena barotrauma telinga tengah yang parah atau manuver Valsava yang kuat.
Manifestasi
Gejala-gejala fistula perilimfa dapat berupa pusing, vertigo, ketidakseimbangan, mual dan muntah. Beberapa orang mengalami telinga berdenging (tinnitus) dan rasa penuh pada telinga, dan banyak yang mengalami gangguan pendengaran. Gejala memburuk dengan perubahan ketinggian (lift, pesawat terbang atau perjalanan di atas gunung), perubahan cuaca dan aktivitas fisik.
Penanganan
Kondisi ini biasanya dapat ditangani secara konservatif dengan istirahat total di tempat tidur dalam posisi duduk. Mengejan, bersin, membuang ingus, aktivitas seksual, suara keras, dan menyamakan telinga tengah harus dihindari untuk mencegah gelombang tekanan di telinga bagian dalam.
Fistula bundar sering kali sembuh secara spontan dalam waktu satu atau dua minggu dengan pengobatan ini, tetapi jika gangguan pendengaran berlanjut atau ciri-ciri lainnya tetap ada, mungkin perlu dilakukan pembedahan untuk memperbaiki kebocoran bundar.
Kebugaran Untuk Menyelam
Bahkan setelah gejala akut fistula oval atau bundar telah sembuh, masa depan penyelam dalam menyelam masih dipertanyakan. Terbang harus benar-benar dihindari selama beberapa bulan untuk memungkinkan penyembuhan cedera atau perbaikan bedah.
Untuk rujukan di daerah Anda, email , atau hubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Pencegahan
Pastikan saluran Eustachius berfungsi dengan baik sebelum menyelam dengan menyamakannya secara perlahan di permukaan.
Vertigo Alternobarik
Vertigo alternobarik terjadi selama turun atau naik, atau segera setelah muncul ke permukaan setelah menyelam dan disebabkan oleh stimulasi tekanan yang tidak sama di setiap telinga.
Statistik
Menurut berbagai sumber, hingga 25 persen penyelam mengalami vertigo alternobarik pada suatu waktu.
Mekanisme
Selama pendakian, udara di ruang telinga tengah mengembang, tekanan relatif meningkat, tuba Eustachius terbuka secara pasif, dan gas keluar melalui tuba Eustachius ke nasofaring. Kadang-kadang tuba Eustachius dapat menghalangi aliran udara ini, yang diikuti dengan distensi udara dan sensasi tekanan yang meningkat pada rongga telinga tengah selama pendakian. Jika sumbatan hanya satu sisi dan perbedaan tekanan lebih besar dari 60 sentimeter air, vertigo dapat terjadi karena peningkatan tekanan menstimulasi alat vestibular. Biasanya hal ini akan berkurang dengan pendakian lebih lanjut, karena tekanan diferensial yang meningkat di ruang telinga tengah memaksa untuk membuka tuba Eustachius dan mengeluarkan udara berlebih. Faktor-faktor yang berkontribusi termasuk barotrauma telinga tengah saat turun, alergi, infeksi saluran pernapasan atas (hidung tersumbat) dan merokok.
Manifestasi
Gejala vertigo alternobarik dapat berupa disorientasi, mual dan muntah.
Catatan: Efek disorientasi akibat vertigo saat menyelam sangat berbahaya. Ketidakmampuan untuk membedakan naik dan turun, mengikuti prosedur pendakian yang aman, dan risiko yang terkait dengan muntah menimbulkan bahaya yang signifikan bagi penyelam serta penyelam lain di dalam air.
Penanganan
Saran yang diberikan oleh Dr. Carl Edmonds tentang cara menangani vertigo alternobarik selama menyelam:
"Jika seorang penyelam mengalami sakit telinga atau vertigo selama pendakian, ia harus turun sedikit untuk meminimalkan ketidakseimbangan tekanan dan mencoba membuka tuba Eustachius dengan menahan hidung dan menelan (manuver Toynbee atau manuver penyeimbangan lainnya). Jika berhasil, hal ini akan menyamakan telinga tengah dengan membukanya hingga ke tenggorokan dan mengurangi distensi pada telinga tengah yang terkena.
"Menutup telinga bagian luar dengan menekan tragus (lipatan kecil tulang rawan di depan liang telinga) dan secara tiba-tiba menekan air yang tertutup ke dalam, terkadang dapat memaksa membuka tuba Eustachius. Jika hal ini gagal, cobalah salah satu teknik pemerataan lain yang dijelaskan sebelumnya, dan cobalah naik perlahan-lahan."
Kasus-kasus yang tidak rumit akan sembuh dengan cepat dalam beberapa menit setelah muncul ke permukaan. Jika gejala berlanjut, temui dokter perawatan primer Anda atau spesialis THT. Jangan menyelam jika Anda mengalami masalah pemerataan.
Cedera yang terkait termasuk barotrauma telinga tengah dan barotrauma telinga dalam; vertigo alternobarik dapat terjadi saat turun atau naik, tetapi umumnya dikaitkan dengan barotrauma telinga tengah saat naik (tekanan balik). Kondisi lain seperti DCS telinga dalam atau vertigo kalori (ketika air dingin tiba-tiba masuk ke salah satu telinga) harus disingkirkan.
Kebugaran Untuk Menyelam
Segera setelah semua gejala dan faktor penyebab teratasi, penyelam dapat kembali menyelam.
Pencegahan
Lakukan tindakan untuk pencegahan barotrauma telinga. Hindari tekanan yang tidak sama pada telinga dengan menghindari tudung pakaian selam atau penyumbat telinga yang ketat. Pertahankan kebersihan telinga yang baik. Jangan menyelam jika tidak dapat menyamakan tekanan.
Tekanan Terbalik (Reverse Squeeze)
Tekanan balik adalah barotrauma akibat ketidakmampuan untuk melepaskan tekanan dari telinga tengah saat mendaki.
Mekanisme
Tekanan harus dilepaskan dari telinga tengah saat penyelam naik, atau udara yang mengembang akan membengkak dan bahkan memecahkan gendang telinga. Udara yang mengembang biasanya keluar melalui saluran Eustachius, tetapi jika saluran tersumbat oleh lendir di kedalaman (biasanya akibat pemerataan yang buruk saat turun, menyelam saat hidung tersumbat, atau mengandalkan dekongestan yang hilang di kedalaman), barotrauma dapat terjadi.
Manifestasi
Tekanan, rasa penuh di telinga
Sakit telinga
Vertigo
Penanganan
Saat menyelam: Kadang-kadang salah satu teknik penyetaraan yang digunakan saat turun akan membersihkan telinga Anda saat naik. Mengarahkan telinga yang sakit ke arah bawah juga dapat membantu. Naiklah selambat-lambatnya sesuai dengan pasokan udara Anda. Tekanan yang meningkat biasanya akan membuka tuba Eustachius dan mengurangi tekanan berlebih. Namun, dalam kasus yang jarang terjadi, hal ini dapat bertahan sampai ke atas. Dalam hal ini, Anda harus menahan rasa sakit untuk mencapai permukaan. Beritahu teman Anda, dan tetaplah berada di dekatnya.
Pertolongan pertama: Semprotan dekongestan hidung dapat membantu membuka tuba Eustachius. Evaluasi oleh dokter disarankan jika Anda mengalami vertigo, nyeri yang berkepanjangan, dan telinga terasa penuh.
Kebugaran Untuk Menyelam
Episode yang berulang memerlukan evaluasi THT. Untuk rujukan THT di daerah Anda, kirimkan email ke Medic@DAN.org, atau hubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Pencegahan
Sebelum menyelam, cobalah menyamakan kedudukan di permukaan untuk memastikan fungsi tuba Eustachius memadai.
Baroparesis Wajah
Baroparesis wajah adalah kelumpuhan saraf wajah yang dapat dibalikkan akibat peningkatan tekanan di telinga tengah saat naik pesawat terbang atau setelah menyelam.
Mekanisme
Mans Bell's Palsy
Saraf wajah adalah saraf kranial yang mengontrol otot-otot wajah. Dalam perjalanannya dari otot ke otak, saraf ini melewati saluran di dinding ruang telinga tengah. Perubahan tekanan di ruang tersebut biasanya hanya sedikit atau tidak berpengaruh pada saraf.
Pada beberapa orang, saluran saraf wajah meleset dari dinding tulang dan dipisahkan dari rongga telinga tengah hanya oleh selaput tipis. Jika orang tersebut mengalami tekanan berlebih di telinga tengah yang sama atau lebih besar dari tekanan kapiler, sirkulasi ke saraf wajah akan terhenti, saraf wajah kehilangan fungsinya, dan otot wajah menjadi lumpuh (baroparesis). Hal ini dapat terjadi saat terbang atau menyelam. Untungnya, tekanan di telinga tengah akan kembali normal segera setelah terpapar, sehingga mengembalikan sirkulasi ke saraf dan memungkinkan fungsinya. Baroparesis wajah cenderung kambuh saat terbang atau menyelam berulang kali.
Manifestasi
Gejalanya meliputi mati rasa, parestesia, kelemahan atau bahkan kelumpuhan pada wajah. Sensasi yang berkurang dan wajah terkulai dapat terlihat, umumnya pada satu sisi wajah.
Penanganan
Baroparesis wajah biasanya ditemukan setelah menyelam. Meskipun durasinya singkat dan sembuh secara spontan, pasien harus dievaluasi oleh dokter untuk menyingkirkan kemungkinan penyebab lain, seperti stroke, infeksi, trauma, atau penyakit dekompresi.
Pada kasus yang jarang terjadi pada baroparesis wajah yang berkepanjangan, perawatan mungkin diperlukan. Terdapat bukti eksperimental bahwa tekanan berlebih yang berlangsung lebih dari 3,5 jam dapat menyebabkan kerusakan permanen. Penyelam yang terus mengalami mati rasa dan terkulai pada wajah harus menemui dokter dalam waktu tiga jam.
Kebugaran Untuk Menyelam
Kondisi ini dapat sembuh sendiri dan sembuh secara spontan dalam beberapa jam, tetapi dapat kambuh lagi saat menyelam atau terbang. Kembali menyelam dapat dipertimbangkan jika gejala telah benar-benar sembuh dan telah dipastikan sebagai akibat barotrauma wajah.
Pencegahan
Pelajari teknik pemerataan yang lembut namun efektif. Jangan menyelam saat terjadi kemacetan.
Sindrom Sendi Temporomandibular (TMJ)
Sindrom sendi temporomandibular adalah rasa sakit di dalam dan di sekitar sendi temporomandibular yang disebabkan oleh cengkeraman corong dari alat selam atau pengatur scuba dalam waktu lama.
Statistik
Telah dilaporkan bahwa TMJ terjadi pada 15-20 persen perenang snorkel dan penyelam scuba.
Mekanisme
TMJ adalah peradangan kronis pada sendi rahang tepat di depan telinga. Rasa sakitnya bisa sangat hebat sehingga membuat sulit untuk memegang corong di antara gigi. Kondisi ini diperburuk oleh faktor lokal seperti kelemahan sendi, faktor anatomi, peradangan kapsuler atau otot, atau jenis corong yang digunakan.
TMJ yang berhubungan dengan menyelam dianggap sebagai akibat dari postur mandibula yang maju ke depan oleh corong yang tidak pas dan mengepalkan corong, terutama dengan regulator yang berat. Menyelam dapat memperburuk TMJ yang sudah ada sebelumnya. Rasa sakitnya terkadang cukup parah sehingga menyebabkan penyelam membatalkan penyelaman. Hal ini dapat terjadi pada penyelam pemula yang mengatupkan gigi, terkadang dengan intensitas sedemikian rupa sehingga mereka kadang-kadang menggigit corong.
Manifestasi
Nyeri pada TMJ dan telinga
TMJ mengklik atau krepitus (suara retak atau meletup)
Trismus (ketidakmampuan untuk membuka mulut sepenuhnya) dan gangguan mobilitas TMJ
Pusing (bisa berbahaya jika terjadi di bawah air)
Nyeri otot pengunyahan
Sensasi pengap di telinga
Disfungsi tuba eustachius
Sakit kepala dan nyeri wajah
Penanganan
Saat menyelam: Berusahalah untuk mengendurkan gigitan Anda sambil mempertahankan corong di tempatnya. Jika tidak berhasil, akhiri penyelaman dengan aman, muncul ke permukaan, dan pertimbangkan opsi corong alternatif.
Pengobatan definitif: Jika rasa sakit terus berlanjut, disarankan untuk berkonsultasi dengan spesialis karena solusinya sangat individual. Perawatan meliputi penyesuaian gigitan, penanganan masalah gigi dan penggunaan corong ortodontik. Obat panas dan anti-inflamasi dapat membantu.
Kebugaran Untuk Menyelam
Kembali menyelam dapat dilakukan setelah rasa sakit hilang. Anda juga harus dapat menggenggam corong tanpa rasa sakit.
Pencegahan
Gunakan hanya corong yang pas. Pertimbangkan corong yang disesuaikan. Perbaiki kondisi yang berkontribusi seperti masalah gigi, kecemasan, dan menggemeretakkan gigi (bruxism).
Telinga Peselancar (Surfer's Ear)
Surfer's ear adalah penyempitan saluran telinga luar akibat pertumbuhan tulang yang tidak normal yang disebabkan oleh paparan kondisi dingin dan basah.
Mekanisme
Saluran telinga luar adalah struktur tubular yang menghantarkan suara dan melindungi telinga tengah. Eksostosis adalah kondisi kronis yang ditandai dengan penyempitan bagian dalam liang telinga akibat pertumbuhan tulang. Dinding tulang tumbuh ke luar secara perlahan selama beberapa tahun sebagai respons terhadap iritasi lokal akibat air dingin. Pertumbuhan ini disebut swimmer's nodes dan umum terjadi pada perenang, peselancar, dan penyelam. Kondisi ini tidak berhubungan dengan infeksi dan juga tidak disebabkan oleh infeksi; namun, penyempitan saluran telinga dapat mencegah air mengalir keluar, yang meningkatkan kerentanan terhadap infeksi telinga luar. Pembengkakan tulang terus tumbuh sementara ada paparan air dingin yang terus menerus (seperti yang ditemukan di air laut dan kolam renang luar ruangan di daerah beriklim sedang). Eksostosis sering terjadi pada penggemar aktivitas luar ruangan di usia pertengahan hingga akhir 30-an, tetapi individu yang mengalami paparan air dingin yang signifikan - seperti peselancar, perenang, dan penyelam - dapat mengembangkan kondisi ini lebih awal.
Saluran telinga yang menyempit lebih rentan terhadap penyumbatan oleh kotoran telinga atau kotoran dan lebih rentan terhadap telinga perenang (otitis eksterna). Eksostosis di dasar liang telinga dapat membentuk suatu bah yang menahan kelembapan dan rentan terhadap infeksi. Eksostosis terlihat sebagai penyempitan saluran telinga. Rata-rata liang telinga memiliki lebar sekitar 0,25 inci (7 milimeter). Pertumbuhan tulang dapat menyebabkan penyempitan hingga 0,04 inci (1 milimeter). Tanda-tanda awal termasuk terperangkapnya air dalam saluran telinga setelah berenang. Perangkap kotoran dan infeksi dapat menyebabkan pembedahan.
Manifestasi
Infeksi telinga luar dan kesulitan mengeluarkan air dari saluran telinga luar dapat terjadi berulang. Gejala eksostosis pada kasus lanjut meliputi penurunan pendengaran yang mungkin dikombinasikan dengan peningkatan prevalensi infeksi telinga.
Diagnosis Diferensial
Penyebab lain dari sumbatan saluran telinga luar dapat berupa infeksi atau impaksi kotoran telinga (serumen).
Perawatan
Jika terjadi penurunan pendengaran atau infeksi berulang, eksostosis dapat diangkat melalui pembedahan.
Kebugaran Untuk Menyelam
Eksostosis tidak memengaruhi kebugaran untuk menyelam kecuali jika eksostosis tersebut menutup saluran telinga atau menyebabkan infeksi berulang.
Pencegahan
Kenakan tudung dalam air dingin.
Setelah menyelam, bilas kedua telinga dengan air tawar untuk membersihkan air dan garam yang terkontaminasi.
Jika rentan terhadap infeksi telinga, hembuskan udara hangat ke dalam saluran eksternal menggunakan pengering rambut (berhati-hatilah agar udara tidak terlalu panas).
Jika telinga Anda memiliki kecenderungan alami untuk menumpuk kotoran telinga, periksalah secara teratur, terutama sebelum perjalanan menyelam yang lama.
Telinga Perenang (Swimmer's Ear)
Peradangan atau infeksi akut pada telinga luar (pinna dan liang telinga) yang disebabkan oleh paparan yang terlalu lama pada kondisi basah dan hangat dikenal sebagai swimmer's ear.
Statistik
Otitis eksterna mempengaruhi satu dari 200 orang Amerika setiap tahun dan hadir dalam bentuk kronis pada 3-5 persen populasi. Perenang, peselancar, dan individu lain yang terpapar pada kondisi basah dan hangat memiliki risiko yang lebih tinggi.
Mekanisme
Saluran pendengaran eksternal adalah bukaan tubular antara lingkungan luar dan gendang telinga (membran timpani). Saluran ini ditutupi oleh kulit dan mengeluarkan kotoran telinga (serumen), yang membantu melindungi dari infeksi.
Otitis eksterna, umumnya disebut sebagai telinga perenang, adalah peradangan atau infeksi akut pada saluran pendengaran eksternal, yang mengakibatkan nyeri telinga dan keluarnya nanah.
Kerusakan pada pelindung saluran telinga luar dapat menyebabkan infeksi. Kelembaban yang berlebihan, trauma mekanis, atau kondisi kulit yang mendasari merupakan faktor penyebabnya. Bakteri yang biasanya ditemukan di saluran telinga luar sering kali memicu infeksi. Dengan seringnya direndam, air akan membengkak sel-sel yang melapisi saluran telinga. Akhirnya, sel-sel ini terpisah cukup jauh sehingga bakteri yang biasanya ditemukan di permukaan liang telinga dapat menembus kulit, di mana mereka menemukan lingkungan yang hangat dan mulai berkembang biak. Otitis eksterna lebih mungkin terjadi jika kulit di liang telinga sudah lecet dan pecah-pecah karena kelembapan yang berlebihan akibat mandi atau garukan. Bakteri atau jamur dari air dapat dengan mudah menyerang kulit yang rusak.
Dermatitis seboroik, psoriasis, dan pembersihan kotoran telinga secara berlebihan yang melukai kulit yang melapisi saluran telinga bagian luar dapat meningkatkan kerentanan saluran telinga terhadap infeksi. Kotoran atau serumen yang berlebihan dapat memerangkap air di dalam liang telinga.
Manifestasi
Keluhan utama umumnya adalah rasa gatal yang sering kali disertai rasa sakit, nyeri dan pembengkakan pada liang telinga. Jika tidak ditangani, pembengkakan dapat meningkat hingga ke kelenjar getah bening di dekatnya dan menimbulkan rasa sakit yang cukup parah sehingga menggerakkan rahang menjadi tidak nyaman.
Penanganan
Pertolongan Pertama
Hindari masuk ke dalam air sampai masalahnya hilang.
Gunakan pengering rambut untuk mengeringkan telinga dengan hati-hati setelah Anda mandi (berhati-hatilah agar udara tidak terlalu panas).
Dalam kasus nyeri, obat pereda nyeri yang dijual bebas bisa efektif. Contoh obat tersebut antara lain asetaminofen (Tylenol), ibuprofen (Advil atau Motrin), atau naproxen (Aleve). Baca dan ikuti semua petunjuk pada label.
Perawatan Berhentilah berenang dan menyelam; jadwalkan janji temu dengan dokter Anda. Jangan memasukkan apa pun ke dalam telinga Anda kecuali jika diinstruksikan. Jika Anda menderita diabetes atau mengonsumsi obat yang menekan sistem kekebalan tubuh, swimmer's ear dapat menyebabkan masalah parah yang memerlukan perhatian medis segera.
Penting bagi dokter Anda untuk menyingkirkan tekanan pada telinga bagian luar, otitis media, dan mastoiditis (infeksi pada tulang di belakang telinga).
Kebugaran Untuk Menyelam
Kembali menyelam dapat dilakukan setelah dokter Anda menentukan bahwa infeksi telah terselesaikan.
Pencegahan
Jaga telinga Anda tetap bersih dan kering.
Keringkan telinga dengan handuk setelah berenang atau mandi dengan memiringkan kepala dan menarik daun telinga ke arah yang berbeda saat telinga menghadap ke bawah.
Hindari memasukkan benda - seperti penyeka kapas atau jari Anda - ke dalam liang telinga atau mengeluarkan kotoran telinga sendiri; kedua tindakan tersebut dapat merusak kulit, sehingga berpotensi meningkatkan risiko infeksi.
Anda dapat mengeringkan telinga Anda dengan pengering rambut jika Anda meletakkannya pada pengaturan terendah dan menahannya setidaknya satu kaki (sekitar 0,3 meter) dari telinga.
Bicarakan dengan dokter Anda tentang apakah Anda harus menggunakan tetes telinga berbahan dasar alkohol setelah berenang.
Jika Anda tahu bahwa Anda tidak memiliki gendang telinga yang tertusuk, Anda dapat menggunakan obat tetes telinga yang dijual bebas atau obat tetes telinga pencegahan buatan sendiri sebelum dan sesudah berenang. Campuran satu bagian cuka putih dan satu bagian alkohol gosok dapat membantu mengeringkan dan mencegah pertumbuhan bakteri dan jamur yang dapat menyebabkan telinga perenang. Pada akhir setiap hari menyelam, teteskan lima tetes larutan tersebut ke dalam setiap telinga. Biarkan selama lima menit sebelum mengeringkannya kembali.
Nyeri adalah gejala yang paling umum dari cedera telinga, tetapi gejala yang paling mengkhawatirkan adalah vertigo, tinitus dan tuli akut. Ketiga gejala tersebut dapat disebabkan oleh berbagai kondisi medis akut dan kronis yang mempengaruhi kebugaran untuk menyelam. Onset akut dari gejala-gejala ini sehubungan dengan menyelam dapat mengindikasikan barotrauma telinga bagian dalam atau penyakit dekompresi dan harus segera dievaluasi secara medis.
Vertigo sering dikacaukan dengan pusing, yang memiliki penyebab dan implikasi yang berbeda. Penyelam harus terbiasa dengan gejala-gejala ini sehingga mereka dapat mengenali potensi masalah dan melakukan intervensi dengan tepat.
Mabuk laut adalah suatu kondisi yang mungkin dialami individu ketika berada di platform yang bergerak. Ini melibatkan perasaan umum sakit, pusing, mual dan muntah. Ini juga disebut mabuk perjalanan. Gerakan pasif mengganggu pergerakan cairan di dalam labirin dan mempengaruhi keseimbangan dan keseimbangan seseorang. Ini dilebih-lebihkan ketika otak menerima pesan yang saling bertentangan yang disampaikan dari mata, otot, dan sensor sendi (proprioseptor). Di ruangan tertutup, pemandangan menunjukkan bahwa sekelilingnya diam, sedangkan sinyal dari labirin menunjukkan bahwa tubuh sedang bergerak.
Mabuk perjalanan dapat terjadi saat bepergian dengan kapal, pesawat, kereta api, bus atau mobil. Beberapa orang lebih sensitif daripada yang lain, tetapi jika rangsangan geraknya kuat dan paparannya berlangsung cukup lama, hampir semua individu akan mengalaminya.
Gejala
Gejala mabuk perjalanan termasuk pusing, berkeringat, mual, muntah, dan perasaan tidak nyaman atau sakit secara umum. Gejala dapat menyerang tiba-tiba dan berkembang dari tidak enak badan menjadi berkeringat dingin, pusing dan muntah. Mabuk perjalanan lebih sering terjadi pada wanita dan anak-anak berusia 2-12 tahun. Individu yang menderita sakit kepala migrain juga lebih rentan terhadap mabuk perjalanan. Mabuk perjalanan berlangsung selama gerakan berlangsung. Begitu gerakan berhenti, gejalanya dengan cepat mereda. Beberapa orang merasakan “kaki laut” setelah lama tinggal di laut.
Pencegahan dan Pengelolaan
Jika Anda tahu Anda mengalami mabuk perjalanan atau mungkin rentan terhadapnya, pertimbangkan saran ini:
Di atas perahu: Tetap di dek dan fokus pada cakrawala. Hindari menghirup asap knalpot.
Di dalam mobil: Duduk di kursi depan. Jika Anda penumpangnya, lihatlah pemandangan di kejauhan.
Jangan membaca di kendaraan yang bergerak. Membaca membuat mabuk perjalanan semakin parah.
Hindari makanan berat sebelum menyelam.
Minum banyak air.
Hindari alkohol di malam hari sebelum Anda bepergian.
Jika memungkinkan, berdiri. Duduk atau berbaring dapat membuat kondisi Anda lebih buruk.
Makan kerupuk kering untuk membantu mengatasi perut mual.
Hindari orang lain yang menjadi mual karena mabuk perjalanan.
Perawatan
Mabuk perjalanan dapat diobati dengan produk obat bebas dan resep.
Produk yang dijual bebas: Antihistamin biasanya digunakan untuk mencegah dan mengobati mabuk perjalanan. Efek samping antihistamin adalah kantuk, yang akan menjadi berlebihan ketika alkohol juga dikonsumsi. Mengantuk dapat mempengaruhi keselamatan penyelam.
Produk resep:Patch kulit skopolamin (Transderm Scop) adalah pilihan yang populer. Patch diterapkan ke area kulit di belakang telinga setidaknya delapan jam sebelum paparan dan dapat membantu mencegah mabuk perjalanan hingga tiga hari per patch. Skopolamin dapat menyebabkan mulut kering, penglihatan kabur, mengantuk dan pusing. Pasien dengan glaukoma, pembesaran prostat dan beberapa masalah kesehatan lainnya tidak boleh menggunakan obat ini. Pastikan untuk memberi tahu dokter Anda tentang masalah kesehatan Anda yang ada untuk membantu menentukan obat mana yang paling cocok untuk Anda.
Pengobatan alternatif:Berbagai pengobatan alternatif telah dipromosikan untuk membantu dalam mengurangi atau mencegah mabuk perjalanan. Dalam kebanyakan kasus, bukti kemanjurannya menghilang. Namun, jika Anda memiliki gejala ringan, Anda dapat mencoba produk jahe atau peppermint untuk meredakan gejala tanpa risiko efek samping.
Vertigo
Vertigo adalah perasaan terus-menerus dari gerakan miring, bergoyang, berputar atau berputar dari diri sendiri atau dunia sekitarnya ketika tidak ada yang bergerak.
Vertigo selama atau setelah menyelam adalah gejala umum dari cedera telinga tengah atau telinga dalam. Hal ini sering dikaitkan dengan mual dan dalam kasus yang parah muntah. Jika vertigo terjadi di bawah air, penyelam mungkin tidak dapat membedakan mana yang naik; panik dan muntah dapat menyebabkan tersedak dan tenggelam. Di darat, pasien mungkin tidak bisa duduk atau berdiri
Ada berbagai penyebab vertigo. Dalam menyelam, paling sering disebabkan oleh barotrauma telinga bagian dalam. Hal ini juga dapat terjadi dari stimulasi satu sisi dan bukan yang lain, seperti ketika perbedaan tekanan hanya pada satu telinga yang menyamakan (vertigo alternobarik) atau ketika air dingin masuk ke satu telinga tetapi tidak pada telinga yang lain (vertigo kalori). Vertigo jenis ini menghilang saat kondisinya menjadi seimbang dan tidak meninggalkan efek yang bertahan lama kecuali disorientasi, mual dan muntah yang terkait saat berada di bawah air dapat menyebabkan kecelakaan menyelam.
Vertigo adalah gejala akut cedera vestibular yang mungkin terkait dengan gejala lain, beberapa di antaranya mungkin menjadi kronis. Gejala mungkin termasuk ketidakseimbangan dan disorientasi spasial, gangguan penglihatan, perubahan pendengaran, gerakan mata yang tidak disengaja (nystagmus), dan perubahan kognitif dan / atau psikologis diantaranya.
Diagnosis Diferensial
Vertigo tidak sama dengan pusing, kepala terasa ringan atau tidak stabil. Saat pusing, Anda mungkin merasa pusing atau kehilangan keseimbangan. Jika Anda merasa ruangan berputar, Anda mengalami vertigo.
Untuk vertigo, bedakan antara penyakit dekompresi telinga bagian dalam (DCS) dan barotrauma telinga bagian dalam.
Pedoman Umum
Vertigo yang terjadi sebentar selama atau setelah menyelam dan sembuh secara spontan memerlukan evaluasi tuba Eustachius sebelum melanjutkan menyelam.
Vertigo yang terus-menerus adalah tanda kondisi serius dan memerlukan evaluasi segera oleh spesialis THT. Untuk rujukan THT di daerah Anda, email Medic@DAN.org, atau hubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Vertigo pasca menyelam persisten yang parah adalah keadaan darurat.
Kebugaran Untuk Menyelam
Kerusakan organ vestibular oleh DCS, barotrauma atau syok akustik mungkin permanen. Dalam kasus cedera telinga tunggal, vertigo dapat hilang dalam dua hingga enam minggu, karena otak belajar untuk mengkompensasi dan mengabaikan sisi yang rusak, tetapi salurannya tidak akan sembuh. Penyelam akan mengalami kesulitan menjaga keseimbangan dalam kegelapan ketika kehilangan petunjuk visual. Kerusakan pada kedua organ vestibular melemahkan dan dapat membuat aktivitas kehidupan tertentu (seperti mengendarai mobil) menantang atau tidak mungkin.
Vertigo yang terus-menerus atau berulang, bahkan jika dikendalikan oleh obat-obatan, mendiskualifikasi menyelam.
Kembali menyelam setelah barotrauma telinga bagian dalam atau DCS harus dievaluasi secara individual tergantung pada tingkat cedera permanen organ telinga bagian dalam.
Tinitus (Telinga Berdenging)
Tinnitus adalah suara atau dering di telinga.
Tinnitus adalah sensasi suara eksternal yang sebenarnya tidak ada. Tinnitus (telinga berdenging) mempengaruhi sekitar satu dari lima orang dan dapat disebabkan oleh banyak kondisi medis.
Tinnitus adalah sensasi suara eksternal yang sebenarnya tidak ada. Tinnitus (telinga berdenging) mempengaruhi sekitar satu dari lima orang dan dapat disebabkan oleh banyak kondisi medis.
Diagnosis Kemungkinan
Penting untuk menemukan penyebab yang mendasari tinnitus. Tinnitus akut yang terjadi selama atau setelah menyelam kemungkinan terkait dengan barotrauma telinga atau DCS telinga bagian dalam. Jika dikaitkan dengan menyelam, dokter Anda harus menentukan apakah itu barotrauma atau DCS telinga bagian dalam, karena perawatannya tidak sama, dan perawatan yang salah bisa berbahaya.
Kemungkinan penyebab tinnitus lainnya termasuk:
Gegar otak
Kebisingan atau ledakan intensitas tinggi
Infeksi
Infeksi telinga (otitis media)
Tumor
Disfungsi sendi temporomandibular (TMJ)
Benda asing dalam telinga
Abnormalitas vaskular
Penyakit Meniere
Hipertensi
Migrain
Beberapa obat (termasuk aspirin dan kina)
Berbagai keracunan (seperti karbon monoksida, nikotin dan logam berat)
Kebugaran Untuk Menyelam
Jika tinnitus tidak berhubungan dengan menyelam dan masalah yang mendasarinya bukan merupakan kontraindikasi untuk menyelam, tidak ada alasan untuk membatasi penyelaman karena tinnitus itu sendiri.
Gangguan Pendengaran/Ketulian
Kehilangan pendengaran atau tuli adalah kehilangan pendengaran sebagian atau seluruhnya dari garis dasar normal.
Kehilangan pendengaran total atau sebagian dapat terjadi karena berbagai alasan. Ada beberapa penyebab yang berhubungan dengan menyelam termasuk barotrauma, penyakit dekompresi (DCS) dan kerusakan pada telinga bagian dalam.
Gangguan pendengaran dapat diklasifikasikan sebagai konduktif atau sensorineural.
Gangguan pendengaran konduktif melibatkan saluran telinga, gendang telinga dan tulang-tulang kecil tulang-tulang pendengaran telinga tengah; komponen anatomi ini secara mekanis menghantarkan suara ke telinga bagian dalam, tempat sinyal listrik dihasilkan.
Gangguan pendengaran sensorineural melibatkan otak, saraf kranial kedelapan atau telinga bagian dalam.
Diagnosis Kemungkinan
Ada banyak penyebab gangguan pendengaran, termasuk infeksi, saluran telinga tersumbat, barotrauma, obat-obatan, trauma, pecahnya jendela bulat atau oval, stroke, penyakit Meniere, kebisingan dan obat-obatan.
Kebugaran Untuk Menyelam
Meskipun jarang, gangguan pendengaran permanen terkait menyelam akibat barotrauma telinga atau DCS telinga bagian dalam mungkin terjadi. Jika cedera menyebabkan kehilangan atau gangguan pendengaran unilateral permanen (hanya satu telinga), sebagian besar dokter akan merekomendasikan untuk tidak kembali menyelam. Ini sering direkomendasikan karena jika penyelaman berikutnya mengakibatkan cedera pada sisa telinga yang berfungsi, individu tersebut dapat mengalami gangguan pendengaran bilateral permanen. Rekomendasi ini berlaku untuk semua individu monaural (pendengaran satu sisi), terlepas dari penyebab gangguan atau gangguan pendengaran unilateral.
Populasi tambahan yang sering tidak disarankan untuk menyelam atau sangat berhati-hati termasuk mereka yang telah menjalani operasi implan koklea, operasi tulang pendengaran atau perbaikan membran timpani (miringoplasti.) Menyelam menempatkan individu dengan riwayat medis ini pada risiko kerusakan perbaikan bedah, mengakibatkan gangguan pendengaran. Untuk penyelam yang telah menjalani prosedur tersebut atau menderita gangguan pendengaran permanen akibat barotrauma telinga, sangat disarankan untuk sangat berhati-hati, dan konsultasi dengan dokter THT sebelum menyelam sangat disarankan. Untuk referensi di daerah Anda, email Medic@DAN.org, atau hubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Penting untuk disebutkan bahwa gangguan pendengaran bilateral (baik bawaan atau didapat) tidak selalu secara medis menghalangi seseorang untuk menyelam. Namun, dalam kasus gangguan pendengaran bilateral, lingkungan menyelam dapat menimbulkan potensi kesulitan dengan komunikasi permukaan, baik dengan penyelam lain maupun dengan anggota kru. Komunikasi yang terhambat dalam kasus-kasus yang berkaitan dengan lalu lintas kapal, penarikan kembali penyelam dan keadaan tak terduga lainnya dapat mengakibatkan keterlambatan tanggap darurat, cedera atau kematian.
Orang-orang menyadari telinga mereka dalam banyak hal. Mereka mengambil tempat yang menonjol di kepala, dan dengan demikian masalah estetika terkadang bersaing dengan masalah kesehatan. Perlindungan alami kulit saluran telinga melibatkan lilin, yang dalam beberapa kasus dapat menjadi gangguan kesehatan dan menyebabkan masalah medis yang nyata. Beberapa orang menganggap lilin sebagai masalah kebersihan dan berusaha keras untuk menghilangkannya. Hal ini dapat menimbulkan masalah tersendiri.
Aktivitas di luar ruangan, terutama olahraga air, membuat telinga terkena kondisi dingin, basah, dan terlalu hangat, yang dapat merusak telinga. Ada banyak solusi komersial yang diusulkan yang konon akan mengurangi risiko cedera atau kerusakan telinga. Sayangnya, hanya sedikit dari produk-produk tersebut yang telah diuji oleh otoritas kesehatan. Di bagian ini, kita akan membahas kebersihan telinga dan obat-obatan serta penyumbat telinga (perangkat yang tidak kami rekomendasikan untuk penyelam) dan tabung ventilasi telinga.
Memiliki saluran telinga yang bersih penting bagi penyelam. Dalam kasus yang ekstrim, kotoran telinga dapat membentuk sumbat dan menjebak udara antara dirinya dan gendang telinga, yang dapat menyebabkan perforasi membran timpani “eksplosif” yang robek ke luar alih-alih perforasi ke dalam yang lebih umum.
Selain itu, sumbat kotoran telinga dapat mencegah air mendinginkan satu telinga, sementara telinga lainnya secara alami didinginkan oleh air yang mengisi saluran telinga. Perbedaan suhu antara kedua telinga ini menyebabkan vertigo kalori.
Akhirnya, sumbat lilin dapat mencegah drainase yang tepat dari saluran telinga. Kelembaban yang tertahan dapat menyebabkan pelunakan kulit dan membuka jalan menuju infeksi.
Lantas, bagaimana cara membersihkan telinga?
Cara yang Salah
Hindari pembersih berujung kapas. Aplikator ujung kapas dapat mendorong kotoran lebih dalam ke telinga, membuat pembuangan kotoran lebih sulit. Selain itu, ujung aplikator kapas dapat terlepas dan tertinggal di saluran telinga. Dalam beberapa hari ini biasanya menyebabkan infeksi saluran telinga yang parah. Jika ini terjadi, kapas harus diidentifikasi dan dikeluarkan oleh dokter yang berkualifikasi. Jangan pernah mencoba melakukan ini sendiri; Anda bisa merobek gendang telinga Anda.
Penanganan Infeksi Serangga
Terkadang, orang yang tidur di luar ruangan atau yang tinggal di daerah hangat bisa terkena serangga di telinga mereka. Serangga di telinga bisa menjadi pengalaman yang mengkhawatirkan. Untuk menghilangkannya, Anda memerlukan kepala yang dingin, terutama jika serangga tersebut masih bergerak atau menyengat.
Di lapangan, Anda dapat menggunakan alkohol gosok, yang dengan cepat menenggelamkan serangga dan membersihkan saluran telinga. Juga diperbolehkan menggunakan spuit bola yang diisi dengan air sabun hangat (seperti sampo bayi) dan larutan hidrogen-peroksida. Jika ini tidak berhasil, dapatkan bantuan medis segera. Metode yang disukai adalah pengangkatan oleh dokter yang berkualifikasi dengan instrumen khusus dan mikroskop.
Cara yang Benar
Lantas, bagaimana cara membersihkan telinga? Saat Anda mandi, sesekali cuci telinga Anda dengan spuit yang diisi dengan air sabun hangat dan larutan hidrogen peroksida. Dalam perjalanan menyelam, gunakan campuran setengah cuka putih dan setengah alkohol setelah seharian menyelam; ini berfungsi untuk membersihkan dan mengeringkan saluran telinga serta mengubah keseimbangan pH agar area tersebut tidak mudah terkena infeksi bakteri. Ini juga dapat membantu mencegah telinga perenang (otitis eksterna).
Jika Anda kesulitan mengeluarkan air dari telinga, coba gunakan pengering rambut. Sebaiknya angkat telinga ke atas dan ke belakang untuk meluruskan saluran telinga dan kemudian meniupkan udara kering yang hangat ke dalam saluran telinga selama lima menit. Berhati-hatilah untuk memastikan udara tidak terlalu panas.
Ingatlah bahwa perawatan telinga memiliki dasar dan kepentingan yang sama dengan perawatan peralatan menyelam Anda yang lain.
Sumbat Telinga
Penyumbat telinga adalah perangkat yang menyumbat saluran telinga luar. Mereka terutama digunakan untuk memblokir tekanan air pada gendang telinga. Umumnya, penyumbat telinga tidak boleh digunakan oleh penyelam.
Prosedur dalam Praktek
Penyumbat telinga padat standar menciptakan ruang udara yang tidak dapat diseimbangkan saat menyelam, membuatnya umumnya tidak aman untuk menyelam; namun, beberapa penyelam menggunakan penyumbat telinga dalam situasi khusus.
Perhatian utama adalah bahwa tekanan air dapat mengganjal sumbat ke dalam saluran telinga. Jika ini terjadi, ada risiko barotrauma telinga luar. Untuk mengatasi masalah ini, beberapa produsen mempromosikan penyumbat telinga berventilasi, yang memiliki lubang kecil untuk ventilasi antara air dan saluran telinga. Lubang biasanya memiliki katup untuk tekanan tanpa membiarkan air masuk ke saluran telinga.
Sebagian besar produsen penyumbat berventilasi menekankan kemudahan ekualisasi produk mereka dan merekomendasikan agar penyelam sering membersihkan telinga mereka saat mengenakan penyumbat telinga untuk mempertahankan tekanan yang tepat. Namun, pernyataan ini belum diuji secara independen. Tidak ada cukup data atau bukti untuk merekomendasikan penggunaan penyumbat untuk penyelam. Risiko komplikasi di bawah air akibat malfungsi atau pelepasan penyumbat telinga adalah nyata dan berpotensi menempatkan penyelam pada peningkatan risiko cedera.
Tetes Telinga
Obat tetes telinga adalah larutan obat yang ditujukan untuk aplikasi di saluran telinga luar.
Penggunaan Tetes Telinga untuk Profilaksis
Bagi kebanyakan penyelam, obat tetes telinga tidak diperlukan setelah menyelam. Tujuan dari kebanyakan obat tetes telinga adalah untuk mencegah infeksi saluran telinga luar (dikenal sebagai otitis eksterna atau telinga perenang). Infeksi saluran telinga berhubungan dengan kelembaban yang terus-menerus serta trauma kulit lokal, yang dapat terjadi akibat memasukkan kapas atau benda lain ke dalam telinga yang dapat merusak lapisan kulit tipis saluran telinga. Seperti yang sering dikatakan oleh spesialis informasi medis DAN, "Jangan memasukkan sesuatu yang lebih kecil dari siku ke telinga Anda." Kelembaban yang terus-menerus dan trauma kulit lokal dapat memungkinkan pertumbuhan bakteri yang berlebihan dan infeksi.
Obat tetes telinga diformulasikan untuk membantu mengeringkan telinga setelah terpapar dan menurunkan keasaman (pH), membuat saluran telinga luar menjadi lingkungan yang tidak ramah untuk kolonisasi dan infeksi bakteri atau jamur. Bahan umum termasuk asam asetat (bahan aktif dalam cuka), asam borat, aluminium asetat, natrium asetat, alkohol isopropil dan gliserin. Asam mengubah pH, yang menghambat pertumbuhan bakteri; aluminium asetat dan natrium asetat adalah zat, yang mengecilkan jaringan. Isopropil alkohol membantu mengeringkan jaringan, dan gliserin dapat membantu melumasi kulit untuk mencegah pengeringan yang berlebihan.
Untuk penyelam yang terganggu oleh telinga perenang, membilas telinga dengan lembut dengan air tawar setelah setiap penyelaman dapat membantu. Mengeringkan telinga dengan pengering rambut juga dapat membantu, tetapi berhati-hatilah untuk memastikan udaranya tidak terlalu panas.
Penggunaan Obat Tetes Telinga
Obat tetes telinga dapat diresepkan oleh dokter Anda untuk mengobati infeksi atau peradangan pada saluran telinga luar. Tetes ini mungkin mengandung antibiotik dan/atau steroid.
Catatan: Penting untuk tidak memasukkan obat tetes ke dalam saluran telinga jika diduga gendang telinga pecah. Biasanya gendang telinga berfungsi sebagai penghalang ke ruang telinga tengah. Jika pecah, kontaminasi atau obat-obatan yang berbahaya bagi telinga bagian dalam dapat memperoleh akses.
Kebugaran Untuk Menyelam
Tetes telinga profilaksis digunakan untuk mencegah infeksi saluran eksternal selama penyelaman berulang selama berhari-hari. Jika Anda merasakan sakit telinga, Anda harus berhenti menyelam dan memeriksakan telinga Anda. Penyelam yang didiagnosis dengan infeksi telinga atau cedera telinga tidak boleh menyelam sebelum sepenuhnya sembuh dan diizinkan oleh dokter.
Tabung Ventilasi Telinga
Tabung ventilasi telinga adalah tabung kecil yang dimasukkan melalui pembedahan melalui gendang telinga untuk meningkatkan drainase dan pemerataan tekanan.
Prosedur
Tabung ventilasi kecil dapat dimasukkan melalui pembedahan melalui gendang telinga (membran timpani) untuk membantu menghentikan siklus infeksi telinga tengah yang berulang. Proses infeksi menyebabkan pembengkakan dan peradangan di saluran Eustachius, mencegah drainase yang tepat; tabung ventilasi memungkinkan drainase dari telinga tengah sampai saluran Eustachius menjadi normal. Memasukkan tabung ventilasi melalui sayatan kecil di membran timpani (miringotomi) biasanya memperbaiki situasi ini.
Tabung tidak dimaksudkan sebagai implan permanen dan biasanya lepas dengan sendirinya atau dikeluarkan oleh dokter. Sayatan kecil biasanya sembuh segera setelah tabung diangkat. Dalam kasus yang jarang terjadi, lubang kecil mungkin tetap ada jika tabung dibiarkan dalam waktu yang lama. Situasi ini dapat diuji dan paling baik ditangani oleh dokter Anda. Tidak mungkin bahwa tabung masih di tempatnya setelah lebih dari beberapa tahun.
Kebugaran Untuk Menyelam
Menyelam tidak dianjurkan saat tabung terpasang karena akan memungkinkan air masuk ke telinga tengah, berisiko vertigo dan infeksi. Setelah tabung ventilasi dilepas atau keluar, waktu yang cukup untuk penyembuhan harus diberikan (setidaknya enam minggu). Fungsi telinga tengah dan tuba Eustachius harus dipastikan normal sebelum menyelam dapat dipertimbangkan.
Masalah yang lebih besar mungkin jaringan parut pada saluran Eustachius sebagai akibat dari infeksi telinga kronis. Hal ini dapat mempersulit penyamaan telinga bagi penyelam. Saat ini, tidak ada prosedur pembedahan yang dapat memperbaiki tuba Eustachius yang tersumbat sebagian.
Anak-anak dan orang dewasa sama-sama membutuhkan perhatian segera untuk gejala infeksi telinga tengah dan barotrauma. Gejala mungkin termasuk tetapi tidak terbatas pada rasa sakit; telinga berdenging atau menderu (tinnitus); sensasi pendengaran parsial, menurun atau teredam; dan drainase dari saluran telinga.
Telinga dan kemampuan Anda untuk menyamakan tekanan dapat dipengaruhi oleh berbagai penyakit. Pada bagian ini, kami telah memberikan informasi tentang dua kondisi yang sering ditanyakan oleh penyelam: penyakit Meniere dan deviasi septum hidung. Jika Anda memiliki pertanyaan tentang kondisi tertentu yang tidak disorot dalam buku ini, jangan ragu untuk menghubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Penyakit Meniere adalah gangguan yang melibatkan episode berulang dari vertigo, yang mungkin berhubungan dengan muntah, gangguan pendengaran yang berfluktuasi, telinga berdenging (tinnitus) dan sensasi tekanan yang meningkat di telinga.
Kondisi kronis ini mempengaruhi telinga bagian dalam. Ini menyebabkan vertigo dan gangguan pendengaran. Episode vertigo yang melumpuhkan mungkin melibatkan mual dan muntah yang parah. Selain itu, penyakit Meniere dapat meredam atau mengganggu pendengaran. Individu juga mungkin mengalami sensasi peningkatan tekanan di telinga. Sakit kepala migrain juga telah dikaitkan dengan kondisi ini.
Penanganan
Perawatan berfokus pada manajemen gejala. Obat-obatan digunakan untuk mengontrol vertigo dan mual dan muntah terkait. Diuretik kadang-kadang digunakan untuk membantu mengatur kelebihan volume endolimfe (cairan yang terkandung di telinga bagian dalam) yang berhubungan dengan penyakit Meniere.
Konsultasi dengan dokter THT direkomendasikan karena prosedur bedah dapat membantu mencapai penyembuhan. Untuk referensi di daerah Anda, email Medic@DAN.org, atau hubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Kebugaran Untuk Menyelam
Kondisi ini bervariasi. Ini mungkin secara spontan menghilang atau berkembang untuk melibatkan telinga yang lain. Jika Anda berisiko mengalami gejala melumpuhkan seperti vertigo, disorientasi, mual atau muntah, sebaiknya jangan menyelam; jika gejala-gejala ini terjadi di bawah air, mereka dapat menyebabkan kepanikan, tersedak, dan bahkan tenggelam. Selain itu, gejala-gejala ini mungkin dikacaukan dengan cedera terkait penyelaman seperti barotrauma telinga bagian dalam atau penyakit dekompresi telinga bagian dalam.
Septum Menyimpang (Deviated Septum)
Penyimpangan dinding yang memisahkan kedua lubang hidung yang dapat menyebabkan penyumbatan saluran hidung dan sinus adalah septum yang menyimpang.
Septum hidung adalah dinding yang memisahkan kedua lubang hidung. Ketika septum dipindahkan atau melengkung, itu dikenal sebagai septum menyimpang. Umumnya kondisi ini tidak banyak atau tidak ada konsekuensinya dan mungkin tidak diperhatikan; individu yang terkena mungkin mengalami kesulitan menyamakan tekanan. Septum yang menyimpang mungkin ada saat lahir (gangguan bawaan) atau akibat trauma pada hidung. Hal ini sering ditemukan selama pemeriksaan fisik rutin. Kondisi ini telah dikaitkan dengan sinusitis serta barotrauma (sinus dan telinga tengah).
Perawatan
Dekongestan dapat memberikan sedikit kelegaan. Koreksi bedah (septoplasti) biasanya diperuntukkan bagi mereka yang memiliki gejala seperti mendengkur, sumbatan hidung, sinusitis berulang, atau sleep apnea.
Kebugaran Untuk Menyelam
Tidak ada kontraindikasi untuk menyelam dengan septum menyimpang tanpa gejala. Jika terjadi infeksi berulang atau kesulitan menyamakan tekanan, konsultasi THT disarankan. Untuk referensi di daerah Anda, email Medic@DAN.org, atau hubungi Saluran Informasi Medis DAN di +1 (919) 684-2948.
Penyakit Dekompresi
Penyakit dekompresi (DCS) adalah hasil yang tidak diinginkan dari menyelam. Tindakan untuk mengurangi risiko DCS harus menjadi bagian dari setiap penyelaman. Buklet ini memberikan konsep terbaru tentang penyebab dan mekanisme, manifestasi khas, manajemen standar dan pencegahan DCS.
Bab 4 – Mengobati Penyakit Dekompresi Pertolongan Pertama di Lokasi Kejadian Evaluasi Selanjutnya Terapi Oksigen Hiperbarik Rekompresi Dalam Air Sumber Daya Darurat
Bab 5 – Faktor-Faktor yang Berkontribusi pada Penyakit Dekompresi Beban kerja Stres Termal Praktik Optimal Perjalanan Udara Setelah Menyelam Kebugaran Medis dan Fisik Keadaan Hidrasi Campuran Gas Pernapasan Tingkat Karbon Dioksida Paten Foramen Ovale Faktor-Faktor Tambahan
Redaktur Pelaksana: Petar Denoble, MD, DSc Penulis: Neal Pollock, PhD
Bab 1: Pengantar Penyakit Dekompresi
“Salah satu bahaya yang terkait dengan penyelaman bawah air adalah penyakit dekompresi (DCS), yang disebabkan oleh pelepasan gas yang tidak terkendali dari jaringan selama atau setelah kembali ke permukaan.”
Menyelam adalah hobi rekreasi yang populer serta kegiatan dengan berbagai aplikasi praktis di bidang ilmiah, komersial, militer, dan eksplorasi. Meskipun menyelam dapat dilakukan dengan aman, penting bagi semua penyelam — apa pun alasan mereka menyelam — untuk menghargai bahwa lingkungan bawah laut tidak kenal ampun. Masalah mungkin timbul selama penyelaman karena kebugaran medis atau fisik yang tidak memadai, penggunaan peralatan yang tidak tepat, atau pengelolaan lingkungan bertekanan tinggi yang tidak memadai.
Salah satu bahaya yang terkait dengan situasi bertekanan di bawah air adalah penyakit dekompresi (DCS), suatu kondisi yang juga dikenal sebagai "the bends". Bab ini menjelaskan dasar-dasar DCS, sementara bab-bab berikutnya memberikan perincian mengenai manifestasi dan pengelolaannya, faktor-faktor risiko yang dapat mempengaruhi Anda terhadap kondisi tersebut dan langkah-langkah pencegahan yang dapat Anda ambil untuk meminimalkan peluang Anda untuk mengalaminya.
Ketika seorang penyelam terkena lingkungan bertekanan tinggi, gas inert (nitrogen, misalnya) menumpuk di jaringan. Semakin dalam menyelam, semakin cepat penyerapan tubuh, atau "penyerapan" gas tersebut. Ketika penyelam naik arah ini dibalik, dan gas meninggalkan jaringan. Laju naik ke permukaan seorang penyelam harus dikontrol untuk memungkinkan eliminasi yang teratur, atau “pembersihan” dari akumulasi gas. Kecepatan naik yang lambat dilakukan secara terus menerus atau bertahap, biasanya memungkinkan dekompresi yang aman, sedangkan naik yang terlalu cepat setelah akumulasi gas terkadang dapat mengakibatkan DCS.
Tekanan udara meningkat perlahan dari nol pada batas ruang menjadi satu atmosfer (14,7 psi) di permukaan laut; tekanan air meningkat jauh lebih dramatis, menambahkan satu atmosfer tekanan untuk setiap 33 kaki air laut.
Konsentrasi, atau "ketegangan", gas inert terlarut di dalam jaringan tubuh Anda adalah fungsi dari tekanan sekitar — yaitu, tekanan lingkungan di sekitar Anda pada waktu tertentu. Gas inert yang tidak digunakan dalam reaksi metabolisme tubuh Anda biasanya ada dalam keseimbangan dengan lingkungan sekitar Anda — dalam konsentrasi yang sama seperti di udara di sekitar Anda. Jaringan di bawah kondisi seperti itu digambarkan sebagai "jenuh." Perubahan tekanan kecil, seperti yang diciptakan oleh perubahan kondisi cuaca, menghasilkan variasi tekanan kecil dalam gas atmosfer yang kemudian disesuaikan dengan perubahan tekanan gas di jaringan tubuh. Ketika perbedaan tekanan, atau "gradien," dibuat, molekul dari area dengan konsentrasi lebih tinggi mengalir ke area dengan konsentrasi yang lebih rendah sampai keseimbangan tercapai kembali. Karena kita semua terus-menerus mengalami perubahan kecil dan koreksi seperti ini, tegangan gas dalam tubuh kita berada dalam keadaan keseimbangan dinamis, bukan statis — bahkan sebelum menyelam ditambahkan ke persamaan.
Tekanan
Lingkungan penyelaman memberikan beban tambahan yang signifikan pada mekanisme adaptif ini. Inilah alasannya: Tekanan diukur menggunakan unit yang dikenal sebagai "atmosfer". Tidak ada batas fisik yang sebenarnya antara atmosfer bumi dan ruang angkasa, tetapi atmosfer sering dianggap membentang 62 mil (100 kilometer) dari permukaan laut ke tepi luar angkasa. Tekanan yang dihasilkan oleh seluruh kolom gas yang bekerja di permukaan laut ini adalah satu atmosfer, sama dengan 14,7 pon per inci persegi (psi) atau 101,3 kilopascal (kPa). Sebagai perbandingan, perubahan tekanan di bawah air meningkat satu atmosfer untuk setiap 33 kaki air asin dan setiap 34 kaki air tawar. Akibatnya, setiap variasi yang Anda alami dalam tekanan atmosfer permukaan sangat kecil dibandingkan dengan variasi tekanan yang dapat Anda alami saat Anda melakukan perjalanan vertikal di bawah air; ini dapat menciptakan gradien besar dalam penyerapan gas selama Anda turun ke kedalaman dan dalam eliminasi mereka selama Anda naik menuju permukaan.
Pertukaran Gas
Paru-paru Anda berfungsi sebagai penghubung utama antara tubuh Anda dan lingkungan tempat Anda berada pada waktu tertentu. Ketika Anda mengekspos diri Anda pada peningkatan tekanan di bawah air, gas di paru-paru Anda dikompresi. Ini menciptakan gradien dari paru-paru Anda ke aliran darah Anda dan, selanjutnya, dari aliran darah Anda ke jaringan Anda saat mereka diperfusi, atau disuplai, dengan darah beroksigen. Jaringan Anda akan mengambil gas inert sampai gradien dihilangkan, keadaan keseimbangan yang efektif, atau saturasi, dengan tekanan lingkungan sekitarnya. Dibutuhkan eksposur yang lama untuk mencapai saturasi penuh, tetapi begitu tercapai, tinggal lebih lama tidak lebih meningkatkan penyerapan gas atau dekompresi yang diperlukan.
Memprediksi Penyerapan dan Eliminasi Gas
Kompartemen Jaringan
Mekanisme fisiologis alami ini dapat diprediksi oleh serangkaian algoritma matematika berdasarkan "kompartemen paruh waktu" (half-time compartments), yang mendekati pola serapan dan eliminasi eksponensial yang diharapkan dalam berbagai jenis jaringan perfusi. Kunci dari algoritme ini adalah bahwa bagian tubuh yang berbeda mengambil dan menghilangkan gas inert pada tingkat yang berbeda - misalnya, darah dianggap sebagai "kompartemen cepat" dan tulang sebagai "kompartemen lambat". (Istilah "kompartemen" tidak dimaksudkan sebagai referensi yang tepat untuk jaringan ini, melainkan sebagai konstruksi matematis untuk memperkirakan apa yang terjadi di berbagai bagian tubuh.)
Jaringan tercepat adalah paru-paru, yang mencapai keseimbangan hampir seketika. Darah mengikuti dengan kecepatan, lalu otak. Jaringan yang paling lambat adalah jaringan yang perfusinya relatif buruk, seperti ligamen dan tulang rawan, atau yang memiliki kapasitas tinggi untuk penyerapan gas inert, seperti lemak di daerah yang perfusinya buruk. Alasan penggunaan algoritme matematika untuk memperkirakan status jaringan adalah karena saat ini belum praktis untuk mengukur serapan atau eliminasi secara langsung dalam jaringan tertentu.
Untuk jaringan teoretis dengan waktu paruh 10 menit, 50 persen perbedaannya dihilangkan dalam 10 menit pertama, lalu 25 persen dalam 10 menit berikutnya (setengah dari sisa 50 persen), lalu 12,5 persen dalam 10 menit berikutnya. , dan seterusnya.
Sebuah contoh dapat menunjukkan bagaimana algoritma bekerja. Mari kita bayangkan seorang penyelam yang langsung dipindahkan dari permukaan ke kedalaman yang tetap — secara efektif, tekanan yang tetap — dan mari kita katakan bahwa dalam skenario penyelaman khusus ini, kompartemen cepat memiliki waktu paruh lima menit. Dalam kasus seperti itu, lima menit pertama paparan tekanan yang lebih tinggi akan menghasilkan penyerapan gas inert yang cukup untuk menghilangkan setengah dari perbedaan yang dihasilkan oleh gradien tekanan (50 persen, dengan kata lain); ini adalah bagian tercuram dari kurva serapan. Periode lima menit kedua akan menghilangkan setengah dari selisih yang tersisa (25 persen lagi). Periode lima menit ketiga akan menghilangkan setengah dari selisih yang tersisa (12,5 persen); keempat, 6,25 persen; kelima, 3,125 persen; dan seterusnya. Pola eksponensial ini berarti bahwa laju perubahan menjadi semakin lambat seiring dengan menurunnya besaran perbedaan. Contoh menggambarkan kompartemen cepat; waktu paruh untuk kompartemen lambat telah dihitung dalam beberapa algoritme hingga hampir 500 menit. Dalam teori dekompresi, perbedaan mutlak dalam tekanan tidak material — konstruksi paruh waktu yang sama berlaku untuk gradien apa pun. Tanpa pengaruh tambahan pada proses, ekuilibrasi, atau saturasi, akan dicapai dalam periode yang sama dengan sekitar enam waktu paruh. Saat gas larut dalam jaringan, perbedaan antara tekanan eksternal dan tekanan internal berkurang, mengurangi kekuatan pendorong.
Kebanyakan penyelaman tidak berlangsung cukup lama bagi penyelam untuk mencapai kejenuhan — ini dikenal sebagai "bounce dive (turun dan naik dalam seketika)." Selama paparan seperti itu, gradien aliran masuk ada sepanjang fase penyelam turun dan di dasar yang menyebabkan penyerapan gas inert yang berkelanjutan, tentu saja di kompartemen lambat tubuh dan mungkin di kompartemen menengah. Ketika penyelam mulai naik, dan tekanan sekitar mulai turun, gradien mulai berbalik — pertama di kompartemen cepat dan kemudian di kompartemen yang semakin lambat.
Derajat Kejenuhan
Secara efektif, selama dan setelah tiba permukaan, sebagian besar jaringan penyelam akan menjadi jenuh dibandingkan dengan tekanan sekitar. Jika derajat lewat jenuhnya rendah, gas-gas inert dapat berjalan secara teratur dari jaringan perifer tubuh ke dalam darah dan kemudian ke paru-paru, dari mana mereka dapat dihembuskan ke atmosfer. Tetapi jika derajat kejenuhan terlalu besar, eliminasi gas-gas inert menjadi tidak teratur. Dalam hal ini, gelembung gas dapat terbentuk di jaringan tubuh penyelam.
Pembentukan gelembung tidak selalu menimbulkan masalah, tetapi semakin tinggi gradien, atau derajat lewat jenuh, semakin besar kemungkinan tanda dan gejala DCS dapat terjadi.
Ini adalah kesalahpahaman yang berbahaya bahwa gelembung terukur terbentuk setelah semua penyelaman dan tidak penting. Tetapi pada saat yang sama, adalah kesalahpahaman bahwa gelembung yang divisualisasikan dalam aliran darah di dalam dan dari dirinya sendiri menandakan DCS. Pembentukan gelembung gas selama dekompresi merupakan stres yang lebih besar dari optimal dan dapat menyebabkan DCS. Yang terbaik adalah mengikuti profil penyelaman konservatif untuk meminimalkan kemungkinan pembentukan gelembung. Kesulitan terbesar adalah mengetahui apa yang dianggap sebagai "konservatif," karena sebagian besar penyelam tidak pernah dipantau untuk gelembung, dan penyerapan dan eliminasi diubah oleh sejumlah faktor selain profil tekanan-waktu.
Perhitungan kompartemen paruh waktu digunakan untuk menghasilkan prediksi batas paparan untuk berbagai kompartemen hipotetis. Dalam bentuk kertas atau plastik ini dikenal sebagai “tabel selam.” Komputer selam modern memungkinkan panduan yang jauh lebih fleksibel karena mereka dapat terus memantau profil tekanan-waktu dan secara bersamaan menghitung status berbagai kompartemen jaringan teoretis. Namun pada kenyataannya, gambarannya jauh lebih kompleks. Pertukaran gas dipengaruhi oleh lebih dari sekedar profil tekanan-waktu. Jadi, meskipun penting bagi penyelam untuk memahami konsep di balik penghitungan kompartemen paruh waktu, penyelam juga harus mengingat bahwa berbagai faktor dapat memengaruhi penyerapan dan pembuangan gas dan secara efektif mengubah risiko dekompresi. Dengan demikian, tanggung jawab ada pada penyelam untuk tidak terlalu bergantung pada tabel atau perangkat untuk keselamatan.
Bab 2 – Menggunakan Komputer Selam Anda Secara Efektif
“Banyak penyelam yang terkejut ketika gejala DCS terjadi setelah penyelaman yang tampak aman menurut komputer selam mereka. Ingat, model mencerminkan seorang penyelam secara rata-rata, bukan Anda. ”
Dalam beberapa tahun terakhir, komputer selam telah menggantikan tabel selam sebagai sarana utama untuk mengatur profil penyelaman. Komputer selam menawarkan keuntungan karena memungkinkan penyelam untuk secara dinamis menetapkan kompartemen yang berbeda sebagai kompartemen pengontrol, karena kondisi berubah selama penyelaman. Pada kenyataannya, kompartemen dalam perangkat lunak pemodelan komputer selam tidak harus mewakili jaringan tertentu, selama panduan yang diberikan oleh model menghasilkan hasil yang dapat diterima — khususnya, dengan peluang DCS sangat sedikit.
Sementara panduan yang diberikan oleh model dekompresi bisa sangat berguna, penting bagi penyelam untuk mengingat bahwa jadwal penyelaman — apakah itu disajikan dalam tabel tercetak atau di layar komputer selam — terbatas dalam apa yang mereka ukur dan dalam asumsi di mana model itu dibangun. Parameter kompartemen jaringan dapat disesuaikan, atau kompartemen baru dapat ditambahkan ke algoritme, jika pengalaman menunjukkan kekurangan dalam model tertentu — tetapi dalam waktu nyata, perhitungan dibatasi oleh variabel yang sedang diproses. Algoritma dapat memperkirakan batas berdasarkan profil waktu dan tekanan (kedalaman) untuk gas pernapasan tertentu, tetapi tidak dapat menghitung dampak dari berbagai faktor waktu nyata, termasuk status termal, intensitas latihan, kekuatan gabungan, dan sejumlah kecenderungan individu yang saat ini tidak dipahami dengan baik, apalagi diukur dalam dampaknya terhadap stres dekompresi.
Penyelam sering terkejut ketika gejala DCS berkembang setelah penyelaman yang dilakukan dalam batas komputer selam mereka. Penting untuk diingat, meskipun model matematika memprediksi hasil, mereka tidak menjaminnya. Fakta bahwa penyelaman dilakukan dalam batas yang disarankan oleh komputer selam (atau tabel selam) tidak membuat terkena DCS menjadi "tidak mungkin". Algoritme matematika memberikan panduan yang harus dievaluasi dan diatur oleh penyelam yang bijaksana.
Banyak penyelam juga tidak menyadari fakta bahwa komputer selam menggunakan banyak model matematika yang berbeda, atau versi model yang berbeda; tidak ada standar universal. Sebuah pabrikan tunggal bahkan dapat menggunakan lebih dari satu model, mungkin dalam satu jenis komputer. Ini membuatnya sangat sulit untuk menilai nuansa lengkap setiap sistem.
Pedoman Dasar
Ada beberapa panduan dasar yang dapat membantu memastikan penggunaan komputer selam yang aman dan efektif. Pertimbangan berikut dimaksudkan untuk menawarkan wawasan yang ringan tentang apa yang komputer selam Anda bisa — dan tidak bisa — lakukan.
Akan sangat membantu untuk memikirkan komputer selam Anda dengan cara berikut:
Sebagai pesaing bisnis: Kuasai dengan mempelajari kekuatan dan kelemahannya.
Sebagai kencan: Harus dihidupkan agar hubungan dapat berjalan.
Sebagai buddy: Harus ikut turun dan naik kapan saja Anda melakukannya.
Sebagai asisten pribadi: Mengingatkan Anda tentang aturan dan jadwal yang mungkin Anda lupakan.
Sebagai seorang aktor: Melafalkan baris-baris kalimat tanpa harus memahami implikasinya.
Sebagai politisi: Jangan percaya semua yang dikatakannya.
Sebagai pramutamu hotel: Akan membantu Anda melakukan apa yang Anda inginkan — tetapi dengan harga tertentu.
Sebagai orang asing: Ia hampir tidak tahu apa-apa tentang realitas pribadi Anda.
Sebagai pasangan: Apakah cocok dengan teman-teman Anda?
Sebagai reporter berita: Ia akan menyiarkan tentang cucian kotor Anda.
Sebagai alat: Gunakan secara tepat.
Tip dan Trik Spesifik
Tekan Tombol yang Tepat
Anda harus tahu tidak hanya tombol mana yang harus ditekan agar komputer Anda bekerja, tetapi juga model matematika atau turunan model mana yang digunakannya dalam membuat perhitungan dekompresi. Ada rentang model yang mengejutkan, dari konservatif hingga liberal, dan perbedaan ini mungkin tidak terlihat pada pandangan pertama. Misalnya, komputer dapat menetapkan batas konservatif untuk penyelaman awal tetapi batas liberal untuk penyelaman berulang. Yang terbaik adalah mempelajari cukup banyak tentang berbagai model dan turunan yang tersedia sebelum Anda memilih komputer selam, jadi Anda pasti memilih salah satu yang kompatibel dengan tingkat toleransi risiko Anda sendiri. Memilih satu murni berdasarkan keakraban mungkin bukan strategi terbaik. Bahkan jika Anda memiliki hasil yang baik pada penyelaman sebelumnya dengan komputer, itu tidak menjamin bahwa itu akan menjadi yang terbaik untuk penyelaman masa depan Anda. Mengumpulkan pengetahuan membutuhkan komitmen, tetapi perencanaan yang matang untuk keselamatan dekompresi harus menjadi perhatian utama.
Setel dan Nyalakan
Gagal menghidupkan komputer selam Anda (atau membawanya saat menyelam) mungkin terdengar seperti lelucon, tetapi itu memang terjadi dan dapat menimbulkan masalah nyata. Tidak ada komputer yang dapat memperhitungkan profil eksposur dari penyelaman sebelumnya jika tidak ada. Dan model dekompresi apa pun tidak valid kecuali Anda mulai menggunakannya saat Anda "bersih" — sepenuhnya terbebas dari gas dari penyelaman sebelumnya. Jika Anda lupa membawa komputer saat menyelam di awal rangkaian yang berulang, Anda kemudian dibatasi untuk menggunakan tabel selama rangkaian tersebut (dengan asumsi bahwa Anda dapat menghitung secara manual eksposur dari penyelaman yang tidak dipantau). Dan jangan pernah berpikir untuk menggantung komputer Anda pada downline selama interval permukaan dalam upaya untuk mengimbangi melupakannya pada penyelaman sebelumnya; mungkin ada cerita tentang itu terjadi, tetapi itu bukan praktik yang bertanggung jawab.
Gunakan Secara Tepat
Satu-satunya orang yang tidak perlu khawatir tentang membawa komputer selam pada setiap penyelaman adalah orang yang menggunakannya semata-mata sebagai datalogger — yaitu, hanya untuk merekam informasi waktu dan kedalaman alih-alih menghitung profil dekompresi. Ingat, bagaimanapun, bahwa menggunakan komputer Anda hanya untuk mencatat waktu dan data kedalaman berarti Anda masih harus merencanakan semua penyelaman Anda menggunakan tabel selam dan harus menghitung ulang status grup berulang Anda setelahnya, sebagaimana mestinya. Anda tidak dapat bergerak masuk dan keluar dari mengandalkan perhitungan dekompresi komputer Anda kecuali telah merekam semua profil eksposur Anda.
Ingat Keterbatasannya
Komputer selam sangat bagus dalam melakukan perhitungan matematis terprogram, tetapi mereka buta terhadap banyak wawasan yang mungkin Anda miliki sebelum, selama dan di antara penyelaman Anda. Misalnya, komputer selam Anda tidak mengetahui apa pun tentang status kesehatan pribadi Anda, tingkat kebugaran fisik Anda, atau kerentanan individu Anda terhadap stres dekompresi. Ia juga tidak tahu apa-apa tentang tekanan panas atau upaya fisik Anda selama atau di antara penyelaman. Fakta bahwa banyak komputer selam menampilkan suhu air mungkin menunjukkan bahwa tekanan termal diperhitungkan dalam algoritme perangkat. Pembacaan suhu air, bagaimanapun, tidak memberikan informasi yang berguna mengenai tekanan termal, karena penyelam yang membawa perangkat dapat mengenakan apa saja mulai dari pakaian renang hingga pakaian selam tanpa tudung hingga pakaian kering air dingin dengan tudung, sarung tangan, dan pakaian air dingin. pakaian dalam. Lebih penting lagi, belum mungkin untuk secara langsung menghitung dampak perbedaan status termal selama bagian yang berbeda dari penyelaman, bahkan jika komputer dapat mengukur suhu inti dan suhu kulit penyelam di titik-titik utama.
Kita tahu bahwa menjadi hangat (bukannya dingin atau dingin) selama fase kompresi dan dasar penyelaman meningkatkan penyerapan gas lembam (tidak optimal), dan menjadi hangat selama fase dekompresi mendorong eliminasi (optimal). Meskipun tidak praktis bagi penyelam yang menyukai kenyamanan, keamanan dekompresi dioptimalkan dengan menjadi netral atau dingin selama fase penyerapan gas inert saat turun dan waktu dasar dan hangat selama fase eliminasi gas inert saat mendaki. Sementara konsep perubahan termal pada tekanan dekompresi jelas, kita masih bertahun-tahun lagi untuk dapat mengukur efek dunia nyata dari faktor-faktor ini untuk tujuan perencanaan penyelaman. Demikian pula, sementara beberapa komputer dapat melacak konsumsi gas, kami harus banyak belajar sebelum informasi ini dapat dimasukkan secara bermakna ke dalam model dekompresi. Variasi konsumsi udara dapat mencerminkan perbedaan kedalaman penyelaman atau pengalaman penyelam, tingkat kecemasan atau tingkat aktivitas fisik. Intinya adalah bahwa menafsirkan dampak fisiologis yang tepat dari interaksi di antara faktor-faktor yang beragam ini sangat sulit, membutuhkan latihan yang bijaksana oleh para penyelam.
Perhatikan Bacaan Komputer Anda
Penyelam perlu memperhatikan komputer selam mereka jika informasi yang diberikan akan berguna. Sadarilah bahwa bias konfirmasi dapat mendorong perilaku berisiko. "Melarikan diri dengan" paparan berisiko sekali, dua kali atau bahkan berkali-kali pada akhirnya dapat menyusul Anda. Ini mungkin tidak benar-benar aman untuk Anda atau pasangan yang mungkin memiliki tingkat kerentanan yang lebih tinggi terhadap stres dekompresi. Mereka yang tidak terlalu khawatir tentang eksposur mereka akan memiliki ketenangan pikiran yang lebih besar jika mereka memilih komputer yang menggunakan model dekompresi yang sangat konservatif. Penting juga untuk memperhatikan komputer selam Anda. Jika Anda menyelam dengan kelompok, jangan lupa bahwa ada banyak variasi dalam panduan yang diberikan oleh komputer yang berbeda atau komputer dengan pengaturan yang dipilih pengguna yang berbeda. Itu berarti ada keuntungan yang cukup besar dalam menyelam dengan orang lain yang menggunakan komputer dengan model dan pengaturan dekompresi yang serupa, karena jika perbedaan kecil muncul, mengikuti arahan yang paling konservatif kemungkinan tidak akan terlalu membebani kelompok tersebut. Tetapi jika anggota kelompok menggunakan komputer selam dengan model yang sangat berbeda, dan setiap penyelam ingin mengikuti perangkatnya sendiri, hal itu dapat menyebabkan gangguan pada sistem teman.
Jangan Mengandalkan Komputer Anda Secara Buta
Meskipun mengindahkan komputer Anda itu penting, jangan mengambil nasihatnya tanpa berpikir. Profil yang sama terkadang dapat dilakukan tanpa masalah lagi dan lagi, hingga penyelaman yang tidak terbukti aman. Penyelam sering mencoba untuk menyalahkan faktor tertentu, seperti dehidrasi, untuk pengembangan gejala setelah satu penyelaman tetapi tidak yang lain. Pendekatan ini tidak produktif. Rentang variabel yang berperan selama penyelaman jarang identik, dan ada elemen probabilistik terhadap risiko dekompresi — yaitu, peluang dapat berperan dalam manifestasi DCS.
Pendekatan terbaik adalah menghindari ekstrem baik pengunduran diri fatalistik atau fokus sombong pada satu peluru ajaib yang diduga. Ada banyak, banyak langkah kecil yang dapat Anda ambil untuk membuat penyelaman apa pun lebih aman. Yang paling penting adalah untuk tetap berada dalam profil kedalaman waktu yang cukup konservatif dan menambahkan perhentian keselamatan untuk setiap penyelaman. Langkah penting lainnya adalah meminimalkan intensitas latihan Anda dan menghindari kepanasan selama fase penyerapan gas saat menyelam, memilih gas pernapasan yang tepat, berlatih cukup sehingga Anda dapat mengontrol daya apung dengan sempurna, tetap cukup istirahat dan terhidrasi, pilih pengaturan yang lebih konservatif yang dapat disesuaikan pengguna di komputer, dan menyelam dengan pasangan yang memiliki tujuan serupa dan mengikuti praktik serupa. Menambahkan margin keamanan kecil ke setiap langkah dapat membantu memberikan bantalan keamanan yang nyaman. Komputer selam adalah alat yang ampuh, tetapi pengetahuan yang baik tentang fisiologi menyelam, pengkondisian fisik yang baik, dan kepatuhan terhadap praktik yang bijaksana menawarkan perlindungan terbaik bagi penyelam.
Bawa Bersama Anda
Jika Anda mengembangkan gejala DCS, Anda harus membawa komputer Anda saat Anda pergi untuk evaluasi medis. Beberapa fasilitas mungkin memiliki kemampuan untuk mengunduh atau meninjau profil Anda untuk membantu dalam evaluasi kasus Anda. Staf medis pasti akan senang melihat konfirmasi deskripsi Anda tentang peristiwa yang memicu gejala Anda.
“Sementara DCS umumnya dianggap sebagai penyakit gelembung, gelembung itu sendiri mungkin sebenarnya hanya pintu gerbang ke serangkaian konsekuensi dan efek yang kompleks.”
DCS dapat berkembang ketika tingkat kejenuhan penyelam sangat tinggi (atau, dengan kata lain, jika gradien eliminasi sangat curam) sehingga perpindahan gas inert yang terkontrol dari jaringan tubuh ke aliran darah - dan kemudian dari aliran darah ke paru-paru dan paru-paru ke lingkungan — tidak mungkin terjadi. Jika proses pembuangan tersebut tidak memadai, gas inert akan keluar dari larutan dan membentuk gelembung yang dapat merusak jaringan, menghalangi aliran darah, menyebabkan kerusakan mekanis (misalnya pada persendian) dan/atau memicu serangkaian respons biokimia.
Meskipun banyak yang diketahui tentang DCS, mekanisme pembentukannya masih diselidiki. Dan sementara DCS umumnya dianggap sebagai penyakit gelembung, gelembung itu sendiri mungkin hanya pintu gerbang ke serangkaian konsekuensi dan efek yang kompleks.
Bintik-bintik kulit seperti ini adalah karakteristik dari cutis marmorata, suatu kondisi yang dapat memperingatkan kemungkinan perkembangan gejala Tipe 2 yang lebih serius.
Tanda dan Gejala DCS
Serangan kolektif terhadap sistem tubuh dapat menghasilkan DCS simtomatik. Efek utama kondisi ini mungkin terlihat pada jaringan yang terkena secara langsung. Efek sekundernya dapat membahayakan fungsi berbagai jaringan, yang selanjutnya membahayakan kesehatan penyelam.
Kemampuan untuk mengenali tanda-tanda, atau bukti objektif, dan gejala, atau persepsi subjektif, DCS - dan untuk membedakannya dari tanda dan gejala yang kemungkinan kecil terkait dengan DCS - adalah penting. Berbagai sistem klasifikasi telah dibuat untuk DCS. Salah satu pendekatan umum adalah menggambarkan kasus DCS sebagai Tipe 1 atau Tipe 2.
DCS Tipe 1
DCS Tipe 1 biasanya ditandai dengan nyeri muskuloskeletal dan gejala kulit atau kulit ringan. Manifestasi kulit Tipe 1 yang umum termasuk gatal-gatal dan ruam ringan (berbeda dari perubahan warna kulit yang jelas berbintik-bintik atau marmer dan kadang-kadang meninggi — suatu kondisi yang dikenal sebagai cutis marmorata yang dapat menandakan perkembangan gejala DCS Tipe 2 yang lebih serius) . Kurang umum tetapi masih terkait dengan DCS Tipe 1 adalah obstruksi sistem limfatik, yang dapat mengakibatkan pembengkakan dan nyeri lokal di jaringan sekitar kelenjar getah bening - seperti di ketiak, selangkangan atau di belakang telinga.
Kolase menunjukkan rasa sakit di beberapa bagian tubuh
Gejala DCS Tipe 1 dapat meningkat intensitasnya. Misalnya, rasa sakit mungkin berasal dari rasa sakit ringan di sekitar sendi atau otot dan kemudian bertambah besar. Namun, rasa sakit yang terkait dengan DCS biasanya tidak meningkat pada pergerakan sendi yang terkena, meskipun memegang anggota badan dalam satu posisi daripada yang lain dapat mengurangi ketidaknyamanan. Rasa sakit seperti itu pada akhirnya bisa sangat parah.
DCS Tipe 2
Tes Romberg mengevaluasi kontrol postural. Romberg yang diasah, yang mencakup menyilangkan lengan dan meletakkan satu kaki di depan yang lain, lebih sensitif terhadap perubahan keseimbangan statis.
Gejala tipe 2 dianggap lebih serius. Mereka biasanya jatuh ke dalam tiga kategori: neurologis, telinga bagian dalam dan cardiopulmonary. Gejala neurologis mungkin termasuk mati rasa; parestesia, atau sensasi yang berubah, seperti kesemutan; kelemahan otot; gaya berjalan yang terganggu, atau kesulitan berjalan; masalah dengan koordinasi fisik atau kontrol kandung kemih; kelumpuhan; atau perubahan status mental, seperti kebingungan atau kurangnya kewaspadaan. Gejala telinga bagian dalam mungkin termasuk dering di telinga, yang dikenal sebagai "tinnitus"; gangguan pendengaran; vertigo atau pusing; mual; muntah; dan gangguan keseimbangan. Gejala kardiopulmoner, yang umumnya dikenal sebagai "tersedak", termasuk batuk kering; nyeri dada di belakang tulang dada, atau tulang dada; dan kesulitan bernapas, juga dikenal sebagai "dispnea." Keluhan pernapasan, yang biasanya disebabkan oleh beban gelembung yang tinggi di paru-paru, dapat membahayakan kemampuan paru-paru untuk berfungsi — mengancam kesehatan penyelam yang terkena dampak, dan bahkan kehidupan, jika pengobatan tidak segera dicari.
Gejala tipe 2 dapat berkembang dengan cepat atau lambat. Pembentukan yang lambat sebenarnya dapat mengaburkan keseriusan situasi, dengan membiarkan penyangkalan tetap ada. Misalnya, kelelahan dan kelemahan adalah masalah yang cukup umum, terutama jika onsetnya berlarut-larut, sehingga sangat mudah untuk diabaikan. Gejala yang kurang umum, seperti kesulitan berjalan, buang air kecil, mendengar atau melihat - terutama jika onsetnya cepat - terkadang dapat mendorong pengenalan yang lebih cepat tentang adanya masalah. Dapat dikatakan bahwa penyelam pada awalnya enggan untuk melaporkan gejala, meskipun biasanya mereka akan melakukannya jika gejalanya tidak hilang. Ini adalah kekurangan yang harus diwaspadai oleh para penyelam, agar mereka tidak menjadi mangsanya.
Presentasi DCS
Penyajian DCS seringkali idiosinkratik — yaitu, pola “khas”nya dapat berupa atipikal. Dalam beberapa kasus, keluhan utama penyelam yang terkena mungkin mengalihkan perhatian dari gejala yang lebih halus tetapi berpotensi lebih penting. Daftar berikut mengurutkan manifestasi awal DCS, dari yang paling umum hingga yang paling jarang dilaporkan (Vann et al. 2011):
Nyeri, terutama di sekitar persendian
Mati rasa atau parestesia
Kekhawatiran konstitusional - seperti sakit kepala, pusing, kelelahan yang tidak dapat dijelaskan, malaise, mual dan / atau muntah, atau anoreksia
Pusing atau vertigo
Kelemahan motorik
Masalah kulit, atau kulit — seperti gatal, ruam, atau bintik-bintik (“cutis marmorata”)
Ketidaknyamanan otot
Gangguan status mental
Masalah paru - seperti kesulitan bernapas ("tersedak")
Koordinasi terganggu
Penurunan tingkat kesadaran
Gejala pendengaran — seperti mendengar suara yang tidak ada atau kesulitan mendengar
Masalah limfatik — seperti pembengkakan regional
Disfungsi kandung kemih atau usus — seperti retensi urin
Fungsi kardiovaskular terganggu
Menurut tinjauan baru-baru ini, nyeri dan mati rasa, juga dikenal sebagai parestesia, dilaporkan awalnya pada hampir dua pertiga kasus DCS, gejala konstitusional pada sekitar 40 persen kasus, pusing/vertigo dan kelemahan motorik pada sekitar 20 persen, dan gejala gangguan kulit pada sekitar 10 persen (Vann et al. 2011).
Diagnosis Diferensial DCS
DCS adalah cedera menyelam profil tinggi karena potensi keparahannya. Tetapi penyelam perlu mengingat bahwa tidak semua masalah yang berhubungan dengan penyelaman berubah menjadi DCS. Ketika dua atau lebih kondisi memiliki gejala yang tumpang tindih, seperti halnya dengan banyak cedera terkait penyelaman, diagnosis banding adalah proses di mana tenaga medis mencari tahu kondisi potensial mana yang paling mungkin bertanggung jawab atas gejala tersebut.
Istilah penyakit dekompresi (DCI) diciptakan untuk mencakup DCS dan kondisi terkait yang dikenal sebagai emboli gas arteri (AGE), yang terakhir timbul dari barotrauma paru-paru yang memasukkan gas ke dalam aliran darah sistemik. Beberapa kondisi dan keadaan lain yang melibatkan gejala serupa termasuk barotrauma telinga bagian dalam; overinflasi telinga tengah atau sinus maksilaris; gas pernapasan yang terkontaminasi; keracunan oksigen; ketegangan muskuloskeletal atau trauma yang diderita sebelum, selama atau setelah menyelam; keracunan biota laut; edema paru imersi; aspirasi air; dan gangguan neurologis kebetulan, seperti stroke (Vann et al. 2011). Stres termal - terkadang karena panas yang berlebihan, tetapi biasanya karena paparan dingin - juga dapat menyebabkan gejala serupa. Dalam beberapa kasus, riwayat medis yang cermat dapat dengan mudah mengesampingkan satu diagnosis atau lainnya. Misalnya, gejala edema paru imersi sering berkembang di kedalaman. Dalam kasus seperti itu, riwayat yang baik akan mengesampingkan DCS, yang hanya berkembang setelah tekanan dekompresi yang signifikan selama pendakian.
Sangat penting bagi penyelam dengan gejala-gejala ini untuk mencari evaluasi dan dukungan medis. Sementara responden pertama mampu melakukan analisis awal dari individu yang terluka, seperti memberikan penilaian neurologis lapangan, kemampuan non-dokter tidak mendekati keterampilan klinis dan wawasan yang dimiliki oleh spesialis klinis berpengalaman.
“Jika tanda atau gejala yang sesuai dengan DCS berkembang, lakukan pertolongan pertama yang tepat dan hubungi layanan medis darurat terdekat. Untuk bantuan darurat tambahan, hubungi DAN di +1-919-684-9111 (Internasional) atau 021-5085-8719 (di Indonesia).”
Ada beberapa elemen untuk manajemen DCS yang efektif, khususnya evaluasi di tempat dan pertolongan pertama, transportasi dan evaluasi dan pengobatan medis definitif. Siapa pun yang menderita DCS harus mencari evaluasi yang tepat, dan kemungkinan perawatan berkelanjutan, dari dokter yang mengetahui dengan baik tentang masalah medis terkait penyelaman.
Dasar dari pertolongan pertama adalah bantuan hidup dasar. Tindakan pertolongan pertama utama untuk DCS adalah pengiriman oksigen tambahan dalam konsentrasi tertinggi, atau fraksi, yang praktis (Longphre et al. 2007). Fraksi oksigen yang tinggi, jika diberikan dengan cepat dan dalam jangka waktu yang lama, dapat mengurangi atau bahkan menghilangkan gejala DCS, meskipun seringkali hanya sementara jika pengobatan definitif tidak dijamin. Sistem oksigen aliran kontinu, menggunakan masker non-rebreather atau masker saku, sering tersedia di lingkungan menyelam; namun, peralatan tersebut memberikan fraksi oksigen sedang. Fraksi yang jauh lebih tinggi dapat dicapai dengan demand mask, meskipun hanya sesuai untuk individu yang sadar yang dapat bernapas sendiri.
Berbagai masker yang berbeda dapat digunakan dengan sistem oksigen.
Para ahli DAN mengembangkan oksigen rebreather permukaan remote emergency oxygen (REMO2) ini untuk penggunaan pertolongan pertama (Pollock dan Natoli 2007).
Sistem rebreather adalah pilihan lain di tempat kejadian; sistem seperti itu memungkinkan oksigen yang tidak terpakai dalam pernafasan penyelam untuk didaur ulang, atau dihirup kembali. Sebuah peralatan rebreather dengan demikian dapat memberikan fraksi tinggi dengan penggunaan gas minimal dan mungkin terbukti sangat membantu dalam pengaturan di mana pasokan oksigen terbatas (Pollock 2004; Pollock dan Natoli 2007).
Sistem penghasil oksigen kimia — perangkat dengan masa simpan panjang yang mengirimkan oksigen melalui reaksi kimia — mungkin dalam beberapa situasi menjadi satu-satunya pilihan yang tersedia. Namun, jika layanan medis darurat tidak mudah diakses, perangkat tersebut tidak mungkin menyediakan pasokan oksigen yang cukup (Pollock dan Natoli 2010).
Evaluasi Selanjutnya
Pertolongan pertama hanyalah langkah pertama dalam merawat penyelam yang terkena dampak. Siapapun yang telah mengalami gejala yang berhubungan dengan DCS disarankan untuk mencari evaluasi medis berikutnya. Ini harus terjadi bahkan jika gejala penyelam membaik atau hilang setelah pemberian oksigen, karena masalah halus dapat terlewatkan atau gejala dapat kembali setelah pengiriman oksigen dihentikan. Untuk alasan yang sama, disarankan untuk mencari masukan dari spesialis pengobatan selam yang berpengalaman — seseorang yang mengetahui semua nuansa dalam presentasi, arah, dan perawatan DCS.
Terapi Oksigen Hiperbarik
Pengobatan definitif untuk DCS adalah terapi oksigen hiperbarik (HBO), atau pemberian oksigen murni pada tekanan yang jauh lebih tinggi daripada tekanan atmosfer. Terapi HBO mengurangi ukuran gelembung apa pun dan meningkatkan gradien yang meningkatkan pengiriman oksigen dan eliminasi gas inert. Terapi HBO biasanya diberikan di ruang rekompresi (chamber).
Ini adalah ruang hiperbarik monoplace — mampu menampung satu pasien, tanpa personel pendukung di dalam, atau "tender".
Regimen HBO yang umum adalah Tabel Perawatan Angkatan Laut AS 6 (USN 2008). Menurut aturan ini, ruang hiperbarik awalnya diberi tekanan hingga 2,8 atmosfer absolut (ATA), setara dengan tekanan yang ditemukan pada 60 kaki (18 meter) air laut. Pasien menghirup oksigen murni, diselingi dengan periode terjadwal untuk menghirup udara reguler untuk mengurangi risiko keracunan oksigen. Durasi perawatan USN TT6 biasanya hanya di bawah lima jam, tetapi perpanjangan dapat ditambahkan sesuai kebutuhan, berdasarkan respons pasien.
Ini adalah chamber hiperbarik multiplace dan multilock kecil yang dapat menampung banyak pasien plus tender di dalam. Personil atau peralatan dapat dipindahkan ke dalam atau ke luar chamber saat perawatan sedang berlangsung.
Perawatan HBO dapat dilakukan di ruang monoplace, seringkali tabung akrilik berukuran untuk menampung hanya satu pasien, atau di ruang multiplace, berukuran untuk menampung satu atau lebih pasien ditambah satu atau lebih "tender" - yaitu, teknisi atau tenaga medis lainnya . Ruang multilock dirancang untuk memungkinkan pasien, tender, atau peralatan dipindahkan ke dalam dan ke luar ruangan saat perawatan sedang berlangsung.
Arah terapi HBO akan bervariasi sesuai dengan rincian setiap kasus; baik presentasi DCS dan responsnya terhadap pengobatan bisa menjadi istimewa. Resolusi penuh gejala DCS seringkali dapat dicapai dengan satu atau terkadang beberapa perawatan HBO. Namun, dalam beberapa kasus, resolusi tidak akan lengkap, bahkan setelah banyak perawatan. Pendekatan klinis normal adalah melanjutkan perawatan sampai tidak ada perbaikan lebih lanjut yang terlihat pada gejala pasien. Gejala sisa sederhana kemudian akan sering sembuh perlahan, setelah rangkaian pengobatan berakhir. Resolusi penuh dari gejala kadang-kadang bisa memakan waktu berbulan-bulan untuk dicapai dan dalam beberapa kasus mungkin tidak pernah terwujud.
Ini adalah chamber hiperbarik multiplace dan multilock yang besar, di mana beberapa eksposur tekanan dapat dilakukan secara bersamaan.
Rekompresi Dalam Air
Rekompresi dalam air dapat menjadi alternatif untuk chamber rekompresi di lokasi terpencil, jika tidak ada chamber terdekat atau sarana untuk mengangkut pasien dengan cepat ke chamber di tempat lain. Teknik ini melibatkan membawa penyelam ke bawah air lagi, untuk mendorong gelembung gas kembali ke dalam larutan untuk mengurangi gejala dan kemudian secara perlahan mendekompresi dengan cara yang mempertahankan pembuangan gas berlebih secara teratur.
Sementara rekompresi dalam air konsepnya sederhana, hal ini hanya dapat dilakukan dengan sejumlah besar perencanaan, dukungan, peralatan dan personil; kondisi perairan yang sesuai; dan status pasien yang sesuai. Tantangan kritis dapat muncul karena perubahan kesadaran pasien, toksisitas oksigen, suplai gas, dan bahkan stres termal. Sebuah rekompresi dalam air yang gagal dapat meninggalkan pasien dalam kondisi yang lebih buruk daripada upaya yang tidak dilakukan. Komunitas medis dan penelitian terbagi atas kegunaan rekompresi dalam air. Adalah di luar cakupan publikasi ini untuk mempertimbangkan semua faktor yang relevan, tetapi cukup adil untuk mengatakan bahwa mungkin ada lebih banyak situasi ketika rekompresi dalam air tidak boleh dilakukan daripada situasi ketika itu akan menjadi pilihan yang masuk akal.
Sebagai aturan umum, seorang penyelam yang memiliki gejala yang konsisten dengan DCS harus dikeluarkan dari air, dan pertolongan pertama harus diberikan di permukaan, bahkan jika terdapat kemungkinan terjadinya penundaan sebelum sebuah perawatan medis definitif dapat dicari.
Sumber Daya Darurat
Tindakan terbaik, jika tanda atau gejala yang sesuai dengan DCS (atau cedera serius lainnya) berkembang, adalah memulai pertolongan pertama yang tepat dan kemudian segera menghubungi layanan medis darurat (EMS) terdekat. Langkah selanjutnya adalah menghubungi DAN untuk meminta saran mengenai perkembangan perawatan yang tepat. Nomor hotline darurat kami adalah +1-919-684-9111.
Umumnya tidak tepat untuk datang tanpa pemberitahuan di chamber hiperbarik terdekat. Hal ini bisa berarti melewati fasilitas di mana korban mungkin dapat menerima evaluasi yang lebih menyeluruh dan tepat. Ingatlah bahwa tidak semua cedera yang terkait dengan penyelaman adalah DCS, meskipun tampaknya demikian di saat yang menegangkan. Selain itu, chamber di beberapa fasilitas tidak tersedia untuk merawat penyelam setiap saat. Salah satu tantangan di Amerika Utara adalah menyusutnya jumlah chamber hiperbarik yang menerima korban menyelam, terutama di luar jam kerja normal.
Hal utama yang harus diingat adalah bahwa menjalin kontak dengan layanan medis darurat dan DAN dapat memastikan manajemen kasus yang tepat waktu dan tepat. Jika ragu, telepon.
SAAT ANDA MENGHUBUNGI HOTLINE DARURAT DAN
Beri tahu operator bahwa Anda memiliki keadaan darurat penyelaman. Operator akan mengkonfirmasi nama, lokasi dan nomor telepon Anda, dan menghubungkan Anda secara langsung dengan staf medis DAN atau meminta seseorang menelepon Anda kembali secepat mungkin.
Anggota staf medis dapat membuat rekomendasi segera atau menghubungi Anda kembali setelah membuat perjanjian dengan dokter setempat
Anggota staf medis mungkin meminta Anda untuk menunggu melalui telepon saat pengaturan sedang dibuat. Rencana ini mungkin memakan waktu 30 menit atau lebih, karena koordinasi yang rumit sering kali diperlukan. Jika situasinya mengancam jiwa, atur transportasi yang aman bagi penyelam ke fasilitas medis terdekat untuk stabilisasi dan penilaian segera terlebih dahulu. Kemudian hubungi Hotline Darurat DAN untuk konsultasi dengan penyedia medis setempat.
Bahkan jika gejalanya tidak parah dan sembuh sepenuhnya, seorang penyelam yang telah mengalami beberapa kali serangan DCS harus mengambil pertimbangan khusus. Terutama jika DCS berulang mengikuti profil penyelaman yang aman, spesialis medis selam harus berkonsultasi untuk menentukan apakah penyelaman dapat dilanjutkan dengan aman.
DAN EMERGENCY HOTLINE +1 919-684-9111 (Internasional) - 021-5085-8719 (di Indonesia)

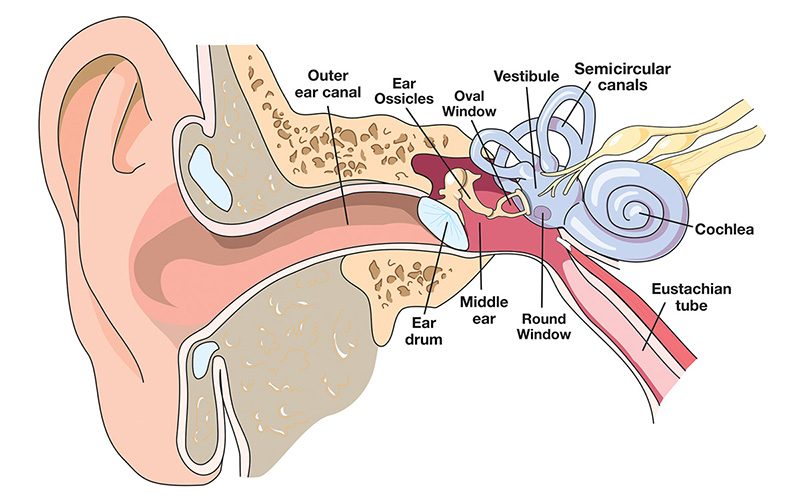
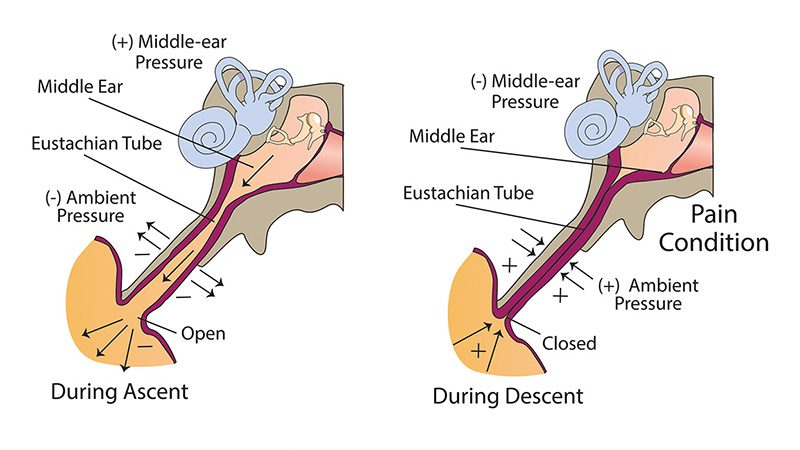



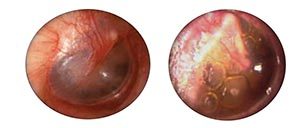

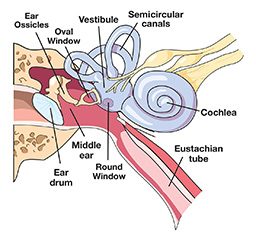
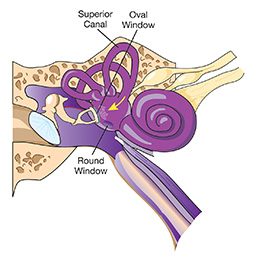



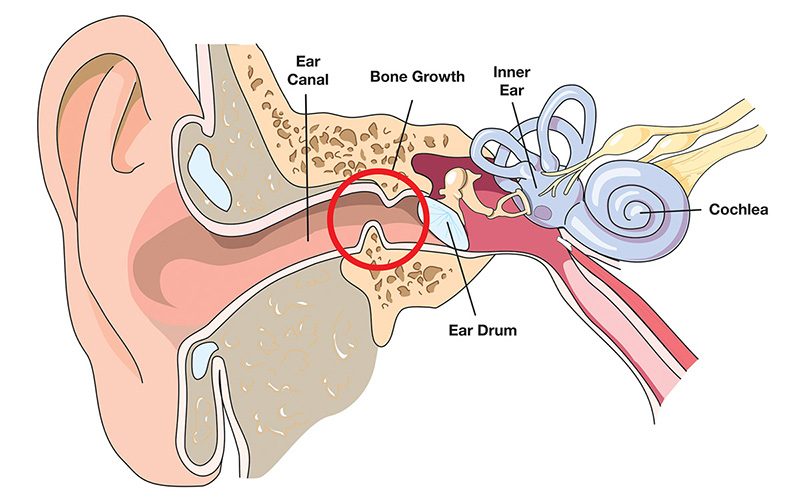












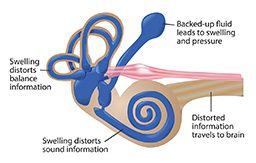
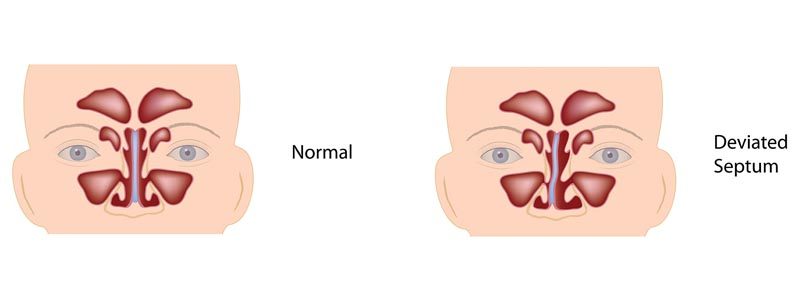


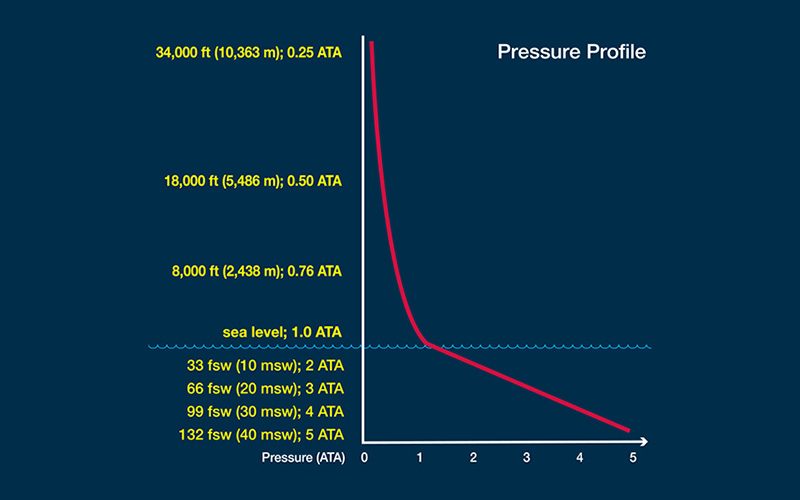
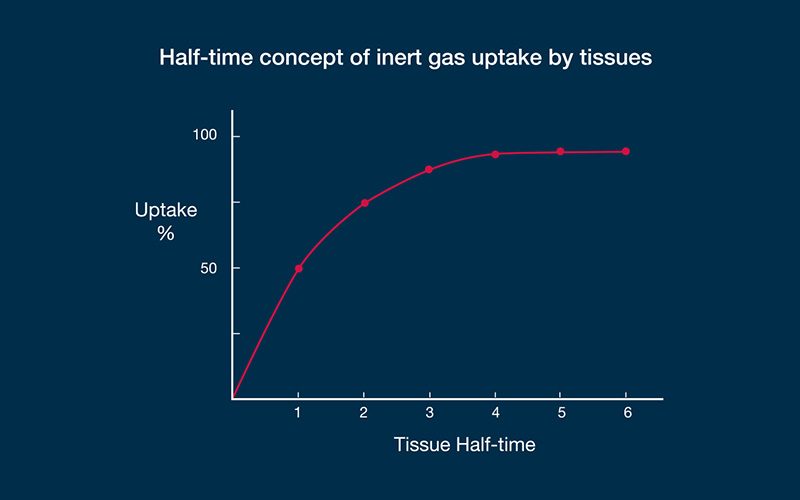

















{kind=link}