
The ear is a complex organ that enables orientation in space, everyday physical activities and social communication. While the anatomy of the ear may be intimidating to some extent, we have tried to provide a simplified but explanatory picture to enhance your comprehension of processes important for diving.
Pressure equalization in the middle ear is the most important skill for divers. If not mastered properly, divers can get injured and sometimes permanently disabled. In divers with healthy ears, ear barotrauma is preventable. Divers should invest time and effort to master equalization techniques.
In this chapter, you’ll learn about:
Anatomy of the Ear
The ear is the organ of hearing and balance. It consists of a cavity in the skull structure lined with soft tissue, which encloses three distinctive spaces filled with air or liquid (external, middle and inner ear); these distinctive spaces host both sound transmission mechanisms and sensory apparatuses.
{kind=link}
Structure
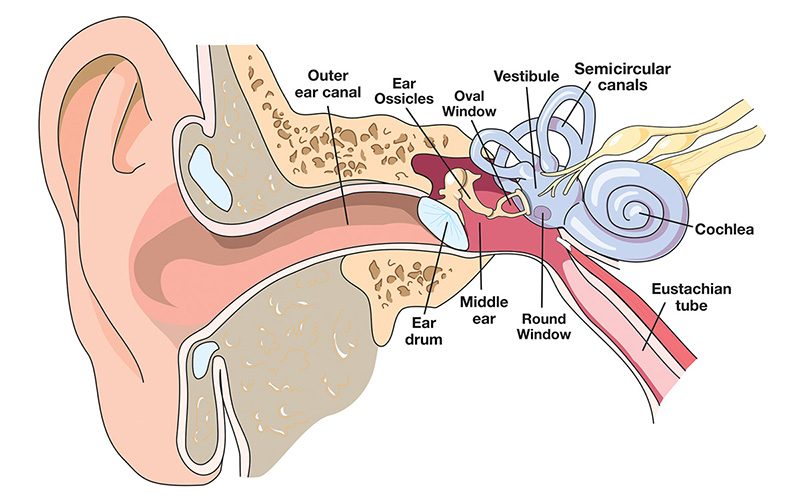
The external ear includes the pinna (auricle) and the ear canal up to the eardrum (tympanic membrane), which separates it from the middle ear. The lining of the external ear is skin rich with glands that produce earwax.
The middle ear is a cavity in a temporal bone lined with a thin layer of tissue similar to that found in the nose and throat. It is separated from the ear canal by the eardrum and connected to the throat via the Eustachian tube. It includes three tiny bones (auditory ossicles) forming the chain attached to the eardrum on one side and to the oval window membrane on the inner-ear side. The middle-ear space is filled with air at ambient pressure, which needs to be equalized when ambient pressure changes (as occurs in diving or flying). This is accomplished by moving air in or out through the Eustachian tubes, which connect the throat to the middle ear, using equalization techniques such as the Valsalva maneuver.
The inner ear, or labyrinth, includes the cochlea (hearing organ) and the vestibule and semicircular canals (balance organs). The cochlea and the vestibule are the origin of the auditory and vestibular nerves.
Function
Pressure waves transmitted by air or water are funneled by the pinna and the ear canal to the tympanic membrane. The pressure waves cause the tympanic membrane to vibrate, which causes the auditory ossicles to move simultaneously in response. The stapes (the last bone in the chain) strikes the oval window of the cochlea. Since this is a closed system, when the oval window is pushed inward, the round window pushes outward. The fluid within the cochlea transmits the pressure waves to the auditory nerve, which in turn, sends signals to the brain that are interpreted as sound.
Parts of the vestibule are projections known as the semicircular canals. The fluid within this system moves correspondingly with head movement. Inside the semicircular canals are hairlike structures called cilia. The cilia detect movement of the fluid through the canals and send the signals through the vestibular nerves to the brain, where the movement is interpreted and used to help determine the position of the head in three-dimensional space.
Middle-Ear Equalization
Middle-ear equalization is a basic, required diver skill that enables the equalization of the pressure in the sinuses and middle-ear spaces with ambient pressure.
Procedure in Practice
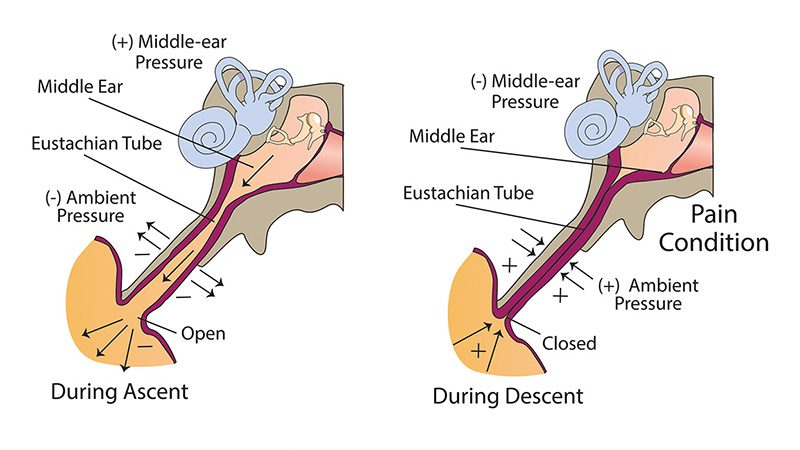
As divers descend in the column of water, environmental pressure increases in a linear fashion at a rate of one-half pound per square inch (PSI) for each foot (0.1 kg/cm2 for each meter) and transmits across the body tissues and fluids. Boyle’s law describes how the volume of the gas decreases when pressure increases, if the amount (mass) of gas and the temperature remain the same. The middle ear is a rigid cavity with the exception of the eardrum. So when pressure increases, the only way for the volume to decrease is the bowing of the eardrum toward the middle-ear cavity (unless gas is added to the space). After the eardrum stretches to its limits, further reduction of middle-ear cavity volume is not possible; if descent continues, the pressure in the middle-ear cavity remains lower than its surroundings. Modest pressure difference will cause leakage of fluid and bleeding from the eardrum and mucosa lining the middle-ear cavity (ear barotrauma O’Neil grade 1). When the pressure difference reaches 5 PSI (0.35 bar), the eardrum may rupture in some divers; at a pressure difference greater than 10 PSI (0.75 bar), rupture will occur in most divers (ear barotrauma O’Neil grade 2). In addition, sudden and large pressure changes may cause inner-ear injury.
So now you understand why during descent you must let more gas into your middle ear to keep the volume of the gas constant and equalize the pressure. A normal middle ear has only one physical communication with the source of additional gas, and that is the Eustachian tube that connects to the nasal cavity (rhinopharynx). Under normal circumstances, the Eustachian tubes are closed, but every time we swallow or yawn, the muscles in our throat allow for a small transient opening that is enough to ventilate our middle ear and compensate pressure.
Nothing challenges our ears and Eustachian tubes more than scuba and breath-hold diving. To become a safe scuba diver and avoid middle-ear injuries, it is essential that you understand the effects of Boyle’s law and learn how to actively let air into your middle ears via the Eustachian tubes. In the following sections, you will find different equalization techniques for you to try.
On ascent, the surrounding pressure decreases and the pressure in the middle remains higher if the gas has no way to leave the middle-ear cavity. When the pressure in the middle ear exceeds surrounding pressure by 15-80 centimeters of water (cm H2O) which corresponds to an ascent in water of 0.5-2.5 feet, the Eustachian tubes open, and surplus gas escapes. If your ears do not equalize at the same rate and the pressure difference reaches about 66 cm H2O (2 feet), vertigo due to unequal pressure stimulus (alternobaric vertigo) may occur.
Upper respiratory tract infections, hay fever, allergies, snorting drugs, cigarette smoking or a deviated nasal septum may compromise equalization. When properly employed, the following techniques are effective in middle-ear and sinus squeeze in healthy subjects.
Equalization Techniques
Passive: Requires no effort. Occurs during ascent.
Voluntary tubal opening: Try yawning or wiggling your jaw. Up to 30 percent of divers can successfully master this technique.
Valsalva maneuver: Pinch your nostrils, and gently blow through your nose.
Toynbee maneuver: Pinch your nostrils and swallow (good technique if equalization is needed during ascent).
Frenzel maneuver: Pinch your nostrils while contracting your throat muscles, and make the sound of the letter “k.”
Lowry technique: Pinch your nostrils, and gently try to blow air out of your nose while swallowing (think Valsalva maneuver meets the Toynbee maneuver).
Edmonds technique: Push your jaw forward, and employ the Valsalva maneuver or the Frenzel maneuver.

Tips for Equalization
- Prior to descent, while you are neutrally buoyant with no air in your buoyancy control device (BCD), gently inflate your ears with one of the listed techniques. This gives you a little extra air in the middle ear and sinuses as you descend.
- Descend feet first, if possible. This allows air to travel upward into the Eustachian tube and middle ear, a more natural direction. Use a descent line or the anchor line to control the speed of descent.
- Inflate your ears gently every few feet for the first 10 to 15 feet.
- Pain is not acceptable. If there is pain, you have descended without adequately equalizing. Ascend a few feet until the pain stops.
- If you do not feel your ears opening, stop and try again; you may need to ascend a few feet to diminish the pressure around you. Do not bounce up and down.
- It may be helpful to tilt the blocked ear toward the surface.
- If you are unable to equalize, abort the dive. The consequences of descending without equalizing could ruin an entire dive trip or cause permanent damage and hearing loss.
- Decongestants and nasal sprays may be used prior to diving to reduce swelling in the nasal and ear passages. If your doctor agrees with your decision to use decongestants, take them one to two hours before descent. They should last from eight to 12 hours, so you don’t need to take a second dose before a repetitive dive. Nasal sprays should be used approximately 30 minutes before descent and usually last 12 hours. Take caution when using over-the-counter nasal sprays; repeated use can cause a rebound reaction resulting in increased congestion and possible reverse block on ascent. Decongestants may have side effects. Do not use them before dive if you do not have previous experience.
- If at any time during the dive you feel pain, experience vertigo or note sudden hearing loss, abort the dive. If these symptoms persist, do not dive again and consult your physician.
Next: Chapter 2 – Injuries >