Proceedings Summary | DAN Flying After Diving Workshop
Introduction
This workshop on flying after recreational diving was organized by Divers Alert Network (DAN) to bring together representatives from the recreational diving industry with experts from other diving communities. The workshop had two purposes: (a) to review the guidelines and experimental data developed since the first flying after diving workshop in 1989; and (b) to debate a consensus for new flying after recreational diving guidelines.
Previous consensus advised to wait 12 hours after a single no-stop dive, 24 hours after multi-day repetitive dive, and 48 hours after dives that required decompression stops. This was considered overly conservative. Subsequently, DAN proposed a simpler 24-hour wait after any and all recreational diving. There were objections to this on the grounds that the decompression sickness (DCS) risks of flying after diving (FAD) were too low to warrant such a long delay and would result in lost business for island diving resorts.
DAN flying after diving trials
Because little human experimental data could be found that was relevant to flying after recreational diving, DAN funded a series of trials at the Duke University Center for Hyperbaric Medicine and Environmental Physiology that were conducted from 1992-1999. Dry, resting volunteers tested nine single and repetitive dive profiles that were near the recreational diving no-decompression limits. The dives were followed by four-hour simulated flights at 8,000 feet (2,438 meters). In 802 trials, there were 40 DCS incidents during or after flight. For single no-stop dives to 60 fsw (feet of sea water; 18 msw, or meters of sea water) or deeper, there was no DCS for surface intervals of 11 hours or longer. For repetitive, no-stop dives, DCS occurred for surface intervals of less than 17 hours. The results of the study were used by the US Navy in 1999 to revise its rules for ascent to altitude following air diving. The new procedures were based on the diver’s repetitive group upon surfacing from a dive and on the expected post-dive altitude. While they were not formally tested in the laboratory prior to issue, no DCS cases have been reported to the Naval Safety Center to date. However, the number of times the new procedures have been used in the field was unknown.
Flying with DCS symptoms
The workshop reviewed recent FAD trials and available field data regarding flying after diving and flying with DCS symptoms. There were potentially important differences between field and chamber studies. Diving in the field involved immersion, exercise, and multiple days of diving, while the chamber trials occurred on a single day with dry resting divers. Thus, the chamber trials might not adequately simulate flying after diving as it actually occurs. As more divers fly with symptoms than develop symptoms during or after flight, flying with symptoms may be a greater health problem than symptoms that occur during or after flight. This is an educational issue, not a scientific issue. Divers need to be taught to seek medical advice rather than to fly if they note signs and symptoms consistent with decompression illness.
Diving nitrox and pre-breathing oxygen reduces risk of DCS in flying after diving

The benefits of oxygen pre-breathing after air diving were confirmed by trials conducted by the Special Operations Command (SOCOM). This organization was concerned with high-altitude parachute operations that might occur after air diving. Flying after diving trials were conducted with dry, resting divers who breathed air while exposed for 60 minutes at 60 fsw (18 msw). Dives were followed by simulated flights of two- or three-hour duration at an altitude of 25,000 feet (7,620 meters). It was demonstrated that this flight may cause DCS even without previous diving. When the dive was followed by a 24-hour surface interval and a three-hour flight, with divers breathing oxygen for 30 minutes immediately preceding flight, during ascent, and while at altitude there was no DCS in 23 trials. The study indicated that: (a) DCS risk was low for these flying after diving exposures, at least for dry resting divers; and (b) preflight oxygen might be an effective means for reducing DCS risk.
Considering possible impact of flying after diving rules on dive operations
One generally thinks of diving guidelines as based on medical safety, but safety is not the only yardstick humans use in establishing rules for living. Economics also has a major impact, albeit one not always articulated with comfort in the medical community. Economics was a primary issue in the 1991 discussion about the impact of DAN’s proposed 24-hour flying after diving guideline. Offshore diving operations felt they would needlessly lose business with a single 24-hour guideline. With this in mind, it was useful to approach the problem of flying after diving with an economic model in which the optimal preflight surface interval was determined by the economic interests of society as represented by divers, resorts, and insurers. Models of this nature depend on their assumptions, and no model can represent all situations, but economic modeling can differentiate between important and unimportant factors. In the model presented, for example, important factors included cost of a dive, number of days diving, aggressiveness of the dive and the DCS risk due to flying after diving. Unimportant factors included the probability of evacuation, the cost of treatment, the diver’s salary and the number of dives per day.
The consensus process
Science is a quantitative activity, while the determination
of safety is a social process that considers the probability,
severity and the costs of injury. Ultimately, the
knowledgeable representatives of society make decisions
about safety for society at large based on available
information. The workshop participants were asked to
reach consensus concerning:
a. whether flying after diving guidelines were needed for recreational diving; (b) whether the current guidelines were adequate;
b. what the longest needed guideline might be; and
c. if shorter guidelines were appropriate
for short dives.
The ensuing discussion determined that guidelines were
needed, and the evidence that had been presented
demonstrated that existing guidelines were inadequate.
After some debate it was decided that unless dive
computers were used, written guidelines for recreational
diving should be simple and unambiguous without the
need for reference to tables such as the U.S. Navy
procedures required. Three groups of divers were
proposed for consideration:
a. uncertified individuals who took part in a “resort” or introductory scuba experience;
b. certified divers who made an unlimited number of no-decompression air or nitrox dives over multiple days; and
c. technical divers who made decompression dives or used helium breathing mixes.
Consensus recommendations for flying after diving
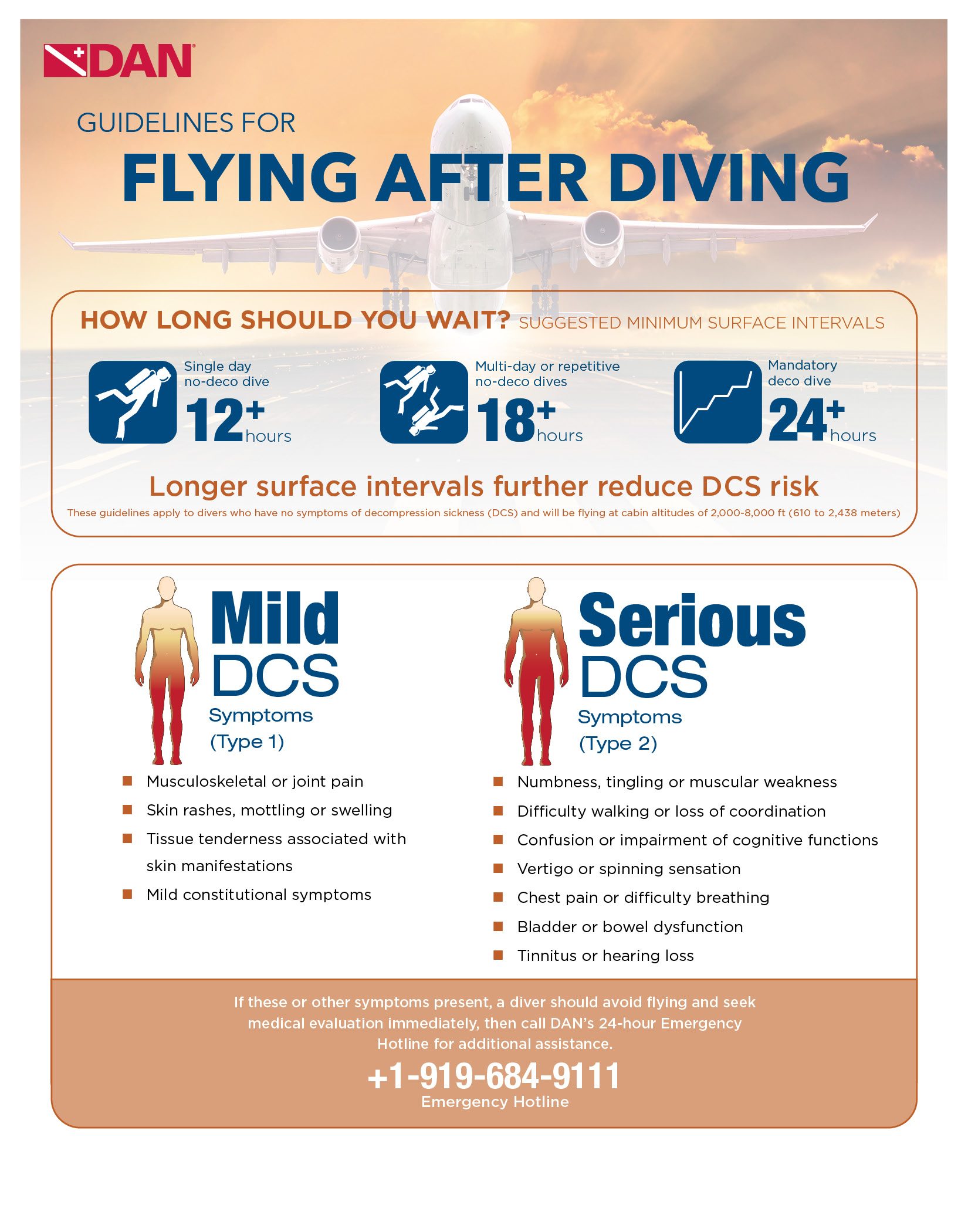
- A minimum of 12-hour surface interval was recommended for the single no-decompression dive.
- A minimum of 18-hour surface interval for multi-day repetitive diving.
- Substantially longer than 18 hours after diving involving compulsory decompression, or using heliox and trimix.
Limitations
It was stressed that as the experimental trials described in the workshop had been conducted in a dry hyperbaric chamber with resting volunteers, longer guidelines might be needed for divers who were immersed and exercising. The effects of exercise and immersion on preflight surface intervals were seen to require experimental study. Additional studies were conducted since and the results will be published soon.
Vann RD. Executive Summary. In: Flying After Diving Workshop. Vann RD, ed. 2004. Durham: Divers Alert Network. ISBN 0-9673066-4-7. 16-19.
Flying After Diving Infographic