DAN® medical information specialists and researchers answer your dive medicine questions.
I RECENTLY UNDERWENT BRAIN SURGERY. The surgery was successful, but now part of my skull has been replaced with mesh. My neurosurgeon is brilliant but does not know how the surgery may affect my diving. Am I still able to dive? Should I limit myself to a certain depth, or should I only snorkel?
While your surgery was successful, returning to diving after this type of surgery may or may not be possible. Clearing someone for diving following brain surgery is a delicate process, and each person needs to be assessed on a case-by-case basis. After any brain surgery, there is a minimum convalescent period that you must observe before considering diving due to an elevated risk of seizure. A seizure in the underwater environment is often fatal, and any increased risk of seizure activity is an absolute contraindication to diving.
As you mentioned, your surgeon may not be familiar with diving and dive medicine. We regularly provide consultations for physicians and encourage medical providers to reach out to us individually to discuss their questions. We are happy to provide information and recommendations so your doctors can make informed decisions about your fitness to dive.
— Ben Strelnick, NREMT, W-EMT
I was born about two months premature. Retinopathy of prematurity was the main complication, and I had oxygen, cryotherapy, and scleral buckles as treatment. I want to take up diving. Is there anything I should be concerned about?
No studies that we are aware of suggest that diving is contraindicated in individuals who have had retinopathy of prematurity. It is important to ensure that at least two months have passed since the surgery and that there is no iatrogenic gas bubble in your eye — retinal surgeons sometimes inject those to facilitate healing after surgery. They remain present for varying lengths of time, depending on the gas the surgeon uses. Residual gas in the eye is an absolute contraindication to diving. It sounds as though none of these considerations apply in your case.

Retinopathy is the primary concern for diving. If your field of vision is greatly affected, this could lead to you being unable to read gauges or properly respond to a situation requiring urgent attention. A diver should be able to do the following:
- Read gauges showing air pressure, depth, dive time, and decompression requirements
- Read a compass
- Locate and navigate entry and exit points
- Locate and recognize their buddy
We recommend you share your intentions for diving with your ophthalmologist as part of getting medical clearance to dive.
—Anne Strysniewicz, AEMT, DMT
I was getting back into diving after a few years off when I was diagnosed with primary myelofibrosis. I have asked my doctors about it, and while they know the disease, I do not think they know about diving’s physiological effects. What concerns should I have about diving?
As you know, myelofibrosis is a rare cancer affecting the bone marrow. The marrow is responsible for producing cells that help our bodies maintain a regular state known as homeostasis. These cells include red blood cells that carry oxygen and blood-clotting factors called platelets. You may want to concern yourself with a few things when deciding if you are fit to dive.
A disruption in red blood cell production may lead to anemia, which can manifest as physical weakness, tiredness, or shortness of breath. Diving is a taxing physical activity from start to finish that includes hauling tanks and gear, donning and doffing gear on a boat, swimming against currents, and climbing a ladder while wearing gear. These exertions may be hazardous to you, and you should consider the risks it can cause for others if you need a rescue. Easy bleeding or bruising are also considerations due to a possible decrease in certain blood cells. Minor bleeding from a fall, a ruptured or perforated eardrum, or barotrauma may be more severe and cause hemorrhaging concerns.
The level of your condition’s malignancy may put you at a greater risk of opportunistic infections, neuropathy, pericardial effusion, and other factors that can lead to convulsions underwater or pulmonary barotrauma.
The effects and side effects of any medications you take are further considerations. While medications metabolize or potentiate faster in hyperbaric environments, you should consider how they make you feel. Pain relief medications can have a narcotic property or create a sedative effect, which can greatly affect your cognitive thinking and how you respond to an unexpected event.
If you are taking medication to treat your condition, side effects can include nausea and vomiting. Some of the signs and symptoms you may experience mimic those of decompression illness and make diagnosing difficult. For a dive trip, you must also be aware of access to emergency care at your location should the need arise.
We can’t determine if you should or should not dive, but we can educate you about the risks you may encounter. Please review this information with your physician along with the RSTC Medical Statement to determine your fitness to dive.
— Robert Soncini, NR-P, DMT

About six weeks ago, I did the Valsalva maneuver to clear my ears after getting off a plane and noticed air coming out the inner corner of my right eye, seemingly from the tear duct. Since then I can feel a puff of air coming out of that spot whenever I blow my nose. I have no other symptoms, but is this anything to be concerned about when I go diving?
What you describe seems to be air passing through your nasolacrimal duct when blowing your nose or trying to equalize by using the Valsalva maneuver. This phenomenon is not uncommon, and some people experience it when they try to equalize too forcefully. You may be executing the Valsalva maneuver with too much force. Equalization should be a gentle and easy process with minimal effort.
While it may feel odd or tickle slightly, you should not have any issues from diving. There is a possibility of infection from forcing mucus from the nasal passage into the nasolacrimal duct.
We recommend consulting a local ear, nose, and throat (ENT) specialist about your concerns. Knowledge of dive medicine is unnecessary as this is a common problem that happens to many people, including nondivers.
— Ben Strelnick, NREMT, W-EMT
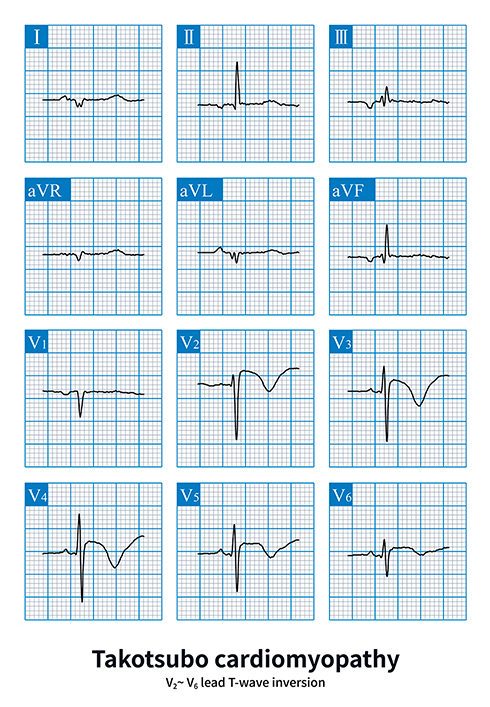
I recently experienced a stress-induced heart attack, and my physician diagnosed me with Takotsubo syndrome. An electrocardiogram showed my heart function returning to normal, and my cardiologist expects a full recovery. What steps should I take, and what should I be aware of before diving again?
Takotsubo cardiomyopathy, or broken heart syndrome, is brought on by stress or strong emotions and can resolve with time. While the symptoms may present like a heart attack, the pathophysiology is quite different.
In a conventional heart attack, a blockage forms at a site of narrowing arteries. This blockage impacts oxygen flow to the heart and can cause infarction (tissue death). With Takotsubo, there is often a lessened blood flow but not a complete blockage, resulting in reduced oxygen to the muscle. Electrocardiograms and blood tests may indicate the patient has suffered a heart attack, but the cardiologist can see no evidence of a blockage. Takotsubo often results in the heart’s left ventricle being enlarged and not working properly.
While Takotsubo cardiomyopathy’s cause is believed to be stress-related, researchers are still investigating the exact mechanism. It may be that the stress triggers an acute inflammation of the heart tissue.
Most patients will start to spontaneously recover within a few hours up to a few days, but the heart muscle takes longer to heal. A 2018 study by Aberdeen University found signs of reduced inflammation five months after a Takotsubo episode. This inflammation may cause long-lasting symptoms, including fatigue, chest pain, and a lack of energy.
The information we have indicates a 10 to 15 percent chance of recurrence, although the trigger may differ. Its recurrence while underwater could prove fatal.
Determining your fitness for a return to diving is much like any diver with a significant cardiac condition, which are all on a case-by-case basis. Your overall well-being and ability to exercise without feeling weak, fatigued, or short of breath are part of it, as are any medications you take and your other medical history.
We recommend close follow-up with your cardiologist during your recovery and waiting to ensure you are completely symptom-free and your exercise tolerance has returned to normal before considering a return to diving. Then you should talk with your cardiologist about your desire to dive, undergo a complete fitness for diving physical, and understand the serious implications if symptoms recur while diving.
Significantly higher in-hospital mortality, hospitalization for stress disorder, and readmission for cardiovascular issues are reported compared to those without this condition.
—Robert Soncini, NR-P, DMT
© Alert Diver — Q3 2022