
“Divers who take drugs to treat cardiovascular diseases often worry about the drugs’ compatibility with diving. However, in most cases, it is the underlying condition and not the drug that should cause concern.”
Some drugs may have side effects that preclude diving. Divers should be very familiar with the side effects of any drugs they take and should discuss them with their physician — and be sure their physician knows about their diving activities. A one-time clearance to dive does not preclude progression of a disease, so any changes in your health status should prompt another medical examination before you dive again.
In this chapter, you’ll learn about:
Antiplatelets and Anticoagulants
Antiplatelets and anticoagulants are two classes of drugs — popularly known as “blood thinners” — that reduce the risk of clot formation and thus the risk of deep vein thrombosis, pulmonary embolism, heart attack and stroke. They may also be prescribed for individuals who have been diagnosed with atrial fibrillation or for those who have had heart-valve surgery or who have received a stent, an implanted pacemaker or an implanted defibrillator. (See other sections for detailed descriptions of these conditions.)
Clots form when blood cells known as platelets stick together, and then proteins in the blood bind them together into a solid mass. Clotting is a normal function that limits and stops bleeding when a blood vessel is injured. However, if a clot grows out of control or starts to travel within the circulatory system, it then poses a danger. Clots may get lodged in a pulmonary artery and cause a pulmonary embolism; in the arteries of the heart and cause a heart attack; or in the vessels of the brain and cause a stroke. All of these events can be life-threatening.

Antiplatelets and anticoagulants keep blood from clotting as quickly or as effectively as usual by preventing the platelets from adhering to one another and by preventing the clotting proteins from binding together. They can even help to break up clots that have already formed.
Antiplatelets — such as aspirin and clopidogrel (also known by the brand name Plavix) — work by preventing the platelets from adhering to one another.
Anticoagulants — such as heparin and warfarin (Coumadin) — inhibit the action of the clotting proteins and thus slow down the chemical reactions that lead to the formation of a clot. There were also several new anticoagulants approved between 2010 and 2012, including rivaroxaban (Xarelto), dabigatran (Pradaxa) and apixaban (Eliquis).
The major side effect of all antiplatelets and anticoagulants is excessive bleeding. Those taking such drugs — especially at too high a dosage — may bleed or bruise easily or may experience bleeding that does not stop as quickly as usual.
Special Caution Regarding Warfarin
Individuals who take warfarin (Coumadin) are generally advised to avoid any activities that may cause abrasions, bruising or cuts — such as contact sports. They are also urged to exercise caution while brushing their teeth and shaving. Even such trivial injuries as insect bites may cause complications in anyone taking warfarin.
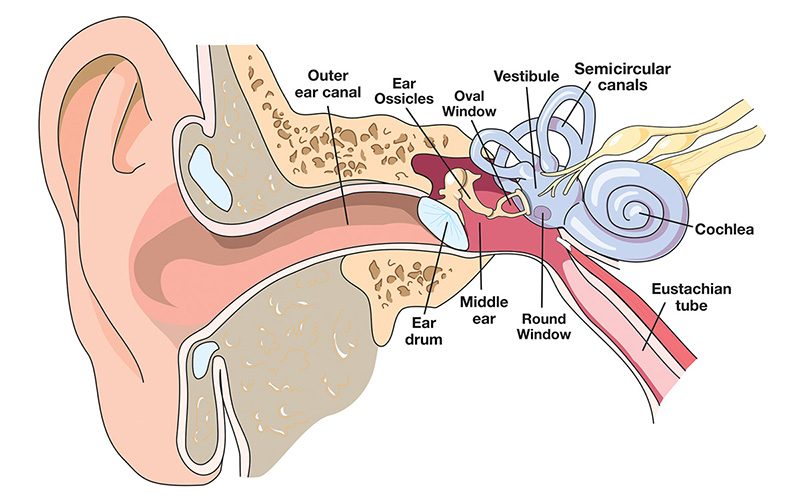
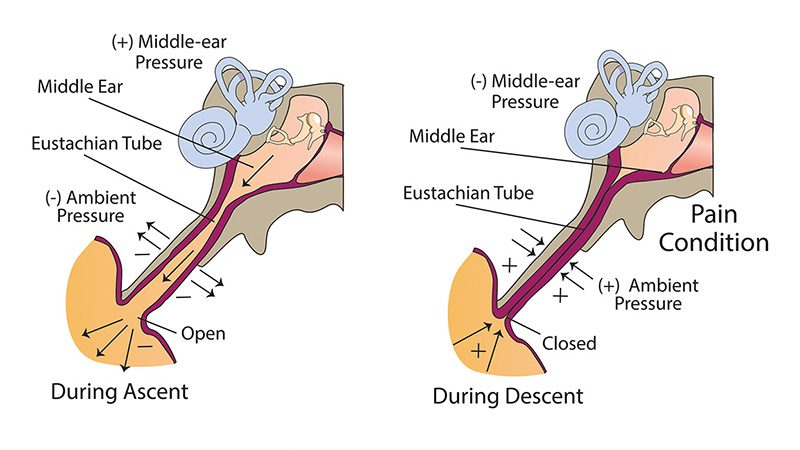
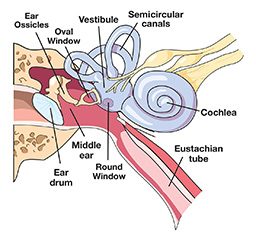
There are additional risks involving warfarin particular to diving. Most significantly, there is an appreciable chance of serious injury in any diving environment, despite one’s best efforts to mitigate the risk. Cuts and bruises are unavoidable, for example. And in anyone taking warfarin, a decompression injury or difficulty equalizing ear pressure could cause bleeding in the ears or the spinal cord that would otherwise not occur.
In addition, both travel and any resulting dietary disruption can interfere with the action of warfarin in dangerous ways. Furthermore, the health-care capabilities in many popular dive destinations may not be up to providing the care that would be required in case of an adverse event.
For all these reasons, anyone taking warfarin is generally advised not to dive. Nevertheless, many people who take warfarin are able to dive without major complications. The keys to safe diving while using warfarin are strict adherence to monthly blood tests and regular surveillance by a physician. With good control of blood-thinning, the risk of a bleeding complication is quite low.
According to Dr. Alfred Bove, a dive-medicine specialist, “For divers, the most important question is whether the condition that requires the use of Coumadin or Plavix prohibits diving. In many cases, the illness is over, or chronic but well adjusted, and does not interfere with safe recreational diving. Safe diving with Coumadin or Plavix depends on the absence of illness that would limit diving, careful control of clotting time, avoiding ear or sinus squeeze, and a thorough education on drugs and foods which cause changes in the effects of Coumadin. There are many divers using Coumadin and Plavix safely, but a special effort must be made to understand how to avoid problems of excess or not enough anticoagulation.”
Statins

Statins are a class of drugs prescribed to lower high blood cholesterol and thus prevent heart attack and stroke. They reduce both LDL cholesterol (“bad cholesterol”) and inflammation in the arteries. Statins work by inhibiting a liver enzyme that is involved in the production of cholesterol. Though they are most effective at lowering LDL cholesterol, they may also contribute to raising HDL cholesterol (“good cholesterol”).
Common statins include the following — listed first by their generic name and, in parentheses, their brand name:
- Atorvastatin (Lipitor)
- Cholestipol (Cholestid)
- Colesevalam hydrochloride (Welchol)
- Fluvastatin (Lescol)
- Lovastatin (Mevacor)
- Ezetimibe (Zetia)
- Ezetimibe combined with simvastatin (Vytorin)
- Fenofibrate (Tricor)
- Pravastatin (Pravachol)
- Rosuvastatin (Crestor)
- Simvastatin (Zocor)
Clinical trials sponsored by the companies that manufacture these drugs have found rare and mild side effects. In a carefully designed trial known as IDEAL, however, almost 90 percent of subjects reported side effects, almost half of them serious. Adverse effects of statins that have been noted in the medical literature and that could interfere with diving include the following:
- Dyspnea (discomfort or difficulty breathing)
- Muscle pain
- Tendon complications
- Digestive problems
- Rash or flushing
- Increased blood sugar or type 2 diabetes
- Cognitive dysfunction (Some studies report that up to 75 percent of those on statins experienced cognitive dysfunction determined to be probably or definitely related to the statin therapy; the severity of the cognitive deficits were clearly related to statin potency.)
- Fatigue (Almost half of those in a 2012 study reported a significant increase in fatigue while taking statins.)
The most common statin side effect is muscle pain. It occurs in about 20 percent of those taking statins. This pain may feel like aches, soreness, tiredness or weakness in your muscles. The pain is sometimes described as mild discomfort, but it is sometimes severe enough to make daily activities difficult. Scientists suspect the occurrence of pain is due to the fact that statins block production of a molecule the body uses to generate energy, called CoQ10; clinical trials are currently exploring whether taking CoQ10 supplements can prevent this side effect. Routine use of CoQ10 supplementation is not recommended, however, even though there are few safety concerns with such supplementation.
Very rarely, statins can lead to a kind of life-threatening muscle damage called rhabdomyolysis; it causes severe muscle pain and may result in liver damage, kidney failure and death. Rhabdomyolysis is especially likely to occur in those who take statins in combination with other drugs such as antibiotics and antidepressants or in those who take a high dose of statins.
Some people who take statins may develop nausea, gas, diarrhea or constipation. These side effects are rare.
A rash or flushing can also occur after taking a statin. This is more likely to occur in individuals who take a statin and niacin together, either in a combination pill such as Simcor or as two separate medications.
The FDA warns on statin labels that some people taking statins have developed memory loss or confusion; these effects are reversed when the medication is halted. Conversely, there has also been evidence that statins may help with brain function — in patients with dementia or Alzheimer’s, for example. This effect is still being studied.
But no matter what side effects individuals taking statins may experience, it is important that they not stop taking the medication without talking to their doctor. It is also important that those who take statins minimize changes in their lifestyle, diet and over-the-counter medications, especially during dive-related travel.
Risk factors for statin side effects include the following:
- Taking multiple cholesterol-lowering medications
- Being 65 or older, female or having a smaller body frame
- Having kidney or liver disease or type 1 or 2 diabetes
- Drinking too much alcohol (more than two drinks a day for men age 65 and younger or more than one drink a day for women of all ages and men older than 65)
In addition, problems are more likely in those who take both statins and the following drugs:
- Antimalarials, such as chloroquine and hydroxychloroquine (Plaquenil)
- Thyroid medications
Effect on Diving
Though the side effects of some statins may interfere with diving, they may nevertheless offer overall health benefits.
One of the effects of statins is an increase in the body’s production of nitric oxide. This helps to preserve the integrity of the endothelium (the inner lining of the blood vessels), to reduce injury from ischemia and/or reperfusion (a procedure that restores circulation after a heart attack or stroke) and to depress interdependent inflammatory and coagulation activity — all of which could provide protection against decompression sickness (DCS). On the other hand, a study of healthy divers who took either a statin or a placebo several days before a dive found no difference in their risk of postdive venous gas bubbles. Thus taking statins specifically to prevent DCS does not appear to offer any benefit, especially in view of the possibility of adverse side effects.
If you are over age 45 and are already taking statins for medical reasons, you need to answer “yes” to at least two questions on the Recreational Scuba Training Council (RSTC) Medical Statement (see the “Physical Activity Recommendations” section for details regarding this form):
Q: Are you presently taking prescription medications? (with the exception of birth control or anti-malarial)?
Q: Are you over 45 years of age and can answer YES to one or more of the following?
- Have a high cholesterol level
These two positive responses signal a pre-existing condition that may affect your safety while diving and that calls for a thorough medical examination to check for the presence of other risk factors or signs of cardiovascular disease. Indeed, anyone who is over age 45, who is at high risk of cardiac problems or who has any signs of cardiovascular disease should see a physician at least once every year.
It is also of note that one-time clearance to dive does not preclude progression of a disease, so any changes in your health status should prompt another medical examination before you dive again. Divers should also be mindful of the fact that they may be required to fill out a new RSTC Medical Statement before any dive and that they may be denied permission to dive based on their responses. However, most dive operators will accept evidence of recent medical clearance for diving. If you are ever in any doubt about your fitness to dive, discuss your status with your dive operator in advance.
Antihypertensives
There are a number of drugs that can be used to lower hypertension (which is also referred to as high blood pressure). Their side effects vary, so some are more suited than others for use by divers.
Beta Blockers

Beta blockers are commonly prescribed to treat hypertension, but they have a big drawback for divers: They can reduce the heart’s capacity for exercise. If a medication restricts the heart’s function during exercise, then there is an increased risk of loss of consciousness, which could prove fatal while diving.
Because of this effect, doctors often recommend that those who take beta blockers undergo a stress test before diving. According to Dr. Alfred Bove, a dive-medicine specialist, divers who take beta blockers but who can achieve a strenuous level of exercise without severe fatigue can be cleared for diving. Bove also points out that although diving does not usually represent the maximum workload on an individual’s heart, anyone who takes beta blockers should avoid extreme exercise because their maximum exercise capacity may be reduced.
ACE Inhibitors
Drugs known as ACE (angiotension-converting enzyme) inhibitors have less effect on exercise capacity than beta blockers, so many doctors prescribe them for people who exercise frequently. But although ACE inhibitors seem to have fewer adverse effects, they can lead to a cough or to airway swelling — conditions that could cause severe problems underwater. If a cough related to ACE-inhibitor use persists, many physicians will recommend a different medication. ACE inhibitors should also be avoided by anyone with kidney disease.
Calcium Channel Blockers
Calcium channel blockers don’t typically pose problems for divers; they relax the walls of the blood vessels, reducing resistance to the flow of blood and thus lowering blood pressure. However, some individuals who take calcium channel blockers, especially in moderate doses, find that a change of position from sitting or lying down to standing causes a drop in blood pressure and thus momentary dizziness. This effect may be cause for concern in divers, but calcium channel blockers appear to have no other adverse implications for diving.
Diuretics
Diuretics reduce the amount of excess water and salt in the body; the decline in the volume of bodily fluids results in a lowering of the blood pressure. Divers seem to have very little trouble with diuretics, although in very warm environments, they may cause excessive water loss and thus dehydration. Because dehydration seems to contribute to the risk of decompression sickness, divers may want to reduce their diuretic dosage on days that they engage in diving — though they should check with their doctor before doing so.
Antiarrhythmics
Antiarrhythmics are designed to help your heart maintain a stable rhythm. Dr. Alfred Bove, a dive-medicine specialist, warns that some antiarrhythmics, when combined with exercise and lowered levels of potassium, could increase the risk of injury to the heart. Although such drugs do not normally interfere with diving, the arrhythmia for which the drug is being taken may itself preclude safe diving. A thorough consultation with a cardiologist and a dive-medicine specialist is essential if you take medication to control an abnormal heart rate and wish to consider diving.
























{kind=link}